The Fetal Thyroid
Amanda Saunders, MD, MBA & Robert Bendon, MD
(All photos are submitted courtesy Dr. Robert Bendon MD, unless otherwise specified)
Internal Examination:
The thyroid may be markedly enlarged in fetuses who receive maternal thyroid stimulating antibodies via placental transfer [1, 2]. This may occur whether or not the mother is euthyroid following thyroidectomy or thyroid suppressive therapy (Fig 1). The fetus may be hydropic from heart failure and cachectic.
The thyroid may also be absent (Fig 1) or sometimes ectopic at the base of the tongue. For this reason, removing the neck block above (cephalad) to the hyoid bone will provide a cross section sample for histologic evaluation of ectopic thyroid tissue. A sample of the thyroid perpendicular to the trachea and including a cross section of the neck organ block often demonstrates the parathyroid as well.

Fig 1: This neg organ block would normally have shown thyroid, but has only muscle. Multiple levels and sections failed to demonstrate thyroid tissue. This 33 weeks of gestation infant of a diabetic mother had 24-48 hours of postmortem retention, and evidence of acute asphyxia. (2x, H&E)
Microscopic evaluation:
Colloid in follicles: Temperature modulation in utero is to a large extent controlled by the mother’s body’s temperature. The developing thyroid does accumulate iodinated protein within variable size follicles. Circulating thyroid hormone in the fetus is mostly reverse T4 which prevents overheating of the fetus in the body-temperature water bath of amniotic fluid. TSH is produced in the fetal hypothalamus and placenta at a basal rate. However, with birth, there is a TSH surge that results in release of active thyroid T3 and T4 that initiates necessary thermogenesis in the fetus [3]. This surge occurs within the first 15 minutes. In sheep, if a lamb is delivered but the attachment of the umbilical cord remains functional to the placenta, the externalized lamb will become hypothermic. Cutting the cord initiates the surge of TSH and epinephrine necessary to maintain body temperature outside the womb.
This histology of loss of follicular colloid in the 24 to 48 hours after birth has been documented in newborn infants at autopsy [4] (Fig 2a-c).

Fig 2a: This thyroid shows normal appearing colloid. Likely there was not a TSH surge in this infant who died of intrapartum asphyxia with severe brain necrosis at 29 hours of age. (4x, H&E)

Fig 2b: This thyroid shows collapse of follicles following a failed resuscitation after birth due to pulmonary hypoplasia from fetal akinesia sequence in the this 39 weeks of gestation infant. (10x, H&E)

Fig 2c: This thyroid shows collapse of many follicles in this 37 weeks of gestation infant who died at 12 hours of age of a cerebral hemorrhage. (10x, H&E)
In stillborn infants the extent of colloid in the thyroid follicles and mononuclear cells in the follicles varies. Some variability may be due to gestational age differences (Fig 3a, b).

Fig 3a: Only a few peripheral follicles show visible colloid accumulation in this 14 weeks of gestation infant with an intrapartum death with preterm labor. The parathyroid is present. (20X, H&E)

Fig 3b: This thyroid shows more expanded follicles at 20 weeks of gestation than at 14 weeks of gestation, but this intrapartum death appears to have resulted in loss of colloid, possibly due to TSH surge during the birth. (10x, H&E)
Another variable may be the effect of autolysis, but this has not been carefully correlated with postmortem retention intervals. Correlations of thyroid histology with disease in the newborn infant has been studied [5]. There is not a study correlating the changes in colloid with other findings in stillbirth, such as evidence of acute asphyxia or thymic involution.
Follicular epithelium: Normally the epithelium is flat to cuboidal. However, in the presence of thyroid stimulating antibodies, there a decrease in colloid and the epithelium becomes more columnar [6] (Fig 4a,b).

Fig 4a: The thyroid follicles are small and empty. The follicular epithelium shows many tall columnar cells. The mother had a normal pulse rate and no clinical evidence or history of Graves disease or other thyroid abnormality. This 30 weeks of gestation infant had mild hydrops and was at the tenth percentile for body weight, so likely was growth restricted. The infant had loss of basophilia in excess of known fetal retention since there had been a normal ultrasound 2 weeks before death, but complete loss of nuclear basophilia in the kidney and adrenal. The thyroid was large on the routine histologic section and showed features similar to cases with maternal Graves disease. The only maternal medication was Tegretol. The etiology of the thyroid changes was never elucidated, but may have been a genetic error in the infant. (40x, H&E)

Fig 4b: This is a higher magnification image of the thyroid in Fig1b. The arrows point to the high columnar follicular epithelium. (100x, H&E)
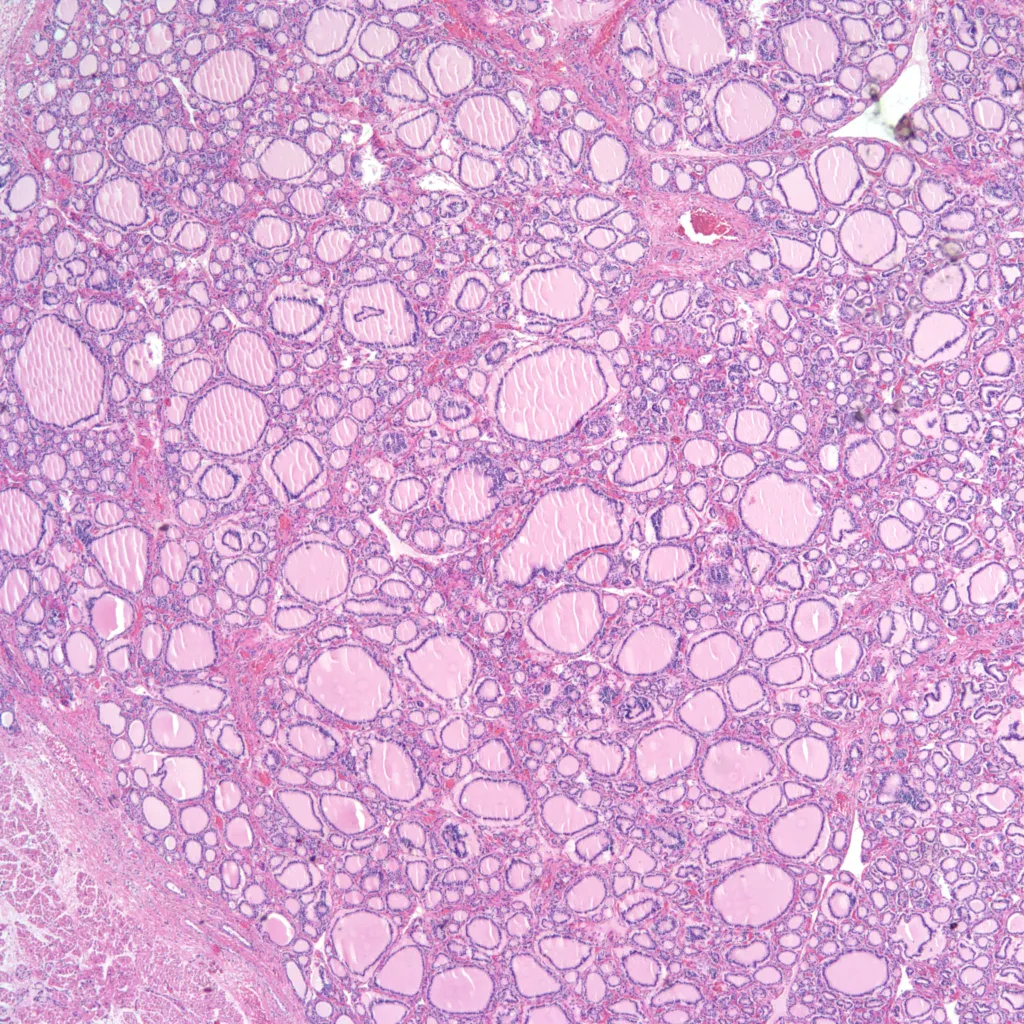
Other abnormalities: The thyroid can have focal clusters of enlarged follicles usually in the context of a maldevelopment syndrome including chromosomal trisomies. (Fig 5a, b).

Fig 5a: Focal enlargement of follicles is present in this 21 weeks of gestation infant with a short rib polydactyly syndrome who survived one hour. (4x, H&E)

Fig 5b: Focal enlargement of follicles is present in this 35 weeks of gestation infant with trisomy 21 with 12 to 24 hours of postmortem retention. (4x, H&E)
References:
1. Munro D, Dirmikis S, Humphries H, Smith T, Broadhead G. The role of thyroid stimulating immunoglobulins of Graves’s disease in neonatal thyrotoxicosis. Br J Obstet Gynecol 1987;85:837-43.
2. Mestman J, Manning P, Hodgeman J. Hyperthyroidism and pregnancy. Arch Intern Med 1974;134:434-9.
3. Abuid J, Stinson DA, Larsen PR. Serum triiodothyronine and thyroxine in the neonate and the acute increases in these hormones following delivery. J Clin Inv 1973;52:1195-9.
4. Sagreiya K, Emery JL. Perinatal thyroid discharge: A histological study of 1225 infant thyroids. Arch Dis Child 1970;45:746-54.
5. Larroche JC. Histological structure of the thyroid gland in the newborn. With special reference to hypotrophy, hydrops fetalis and Cesarean section delivery. Biol Neonate 1976;28:118-24.
6. Skeleton M, Gans B. Congenital thyrotoxicosis, hepatosplenomegaly and jaundice in two infants of exophthalmic mothers. Arch Dis Child 1955;30:460-4.









