
The Fetal Kidney
Amanda Saunders, MD, MBA & Robert Bendon, MD
(All photos are submitted courtesy Dr. Robert Bendon MD, unless otherwise specified)
Internal Examination:
The kidneys are visible from the posterior organ block. The location, amount of fat, color, and the hilar connection of the ureters, renal artery and renal vein should all be noted.
Absent kidneys: Absent kidneys occurs with multiple genetic pathways. Beside the obvious lack of the kidneys, the distortion of the overlying adrenal glands also is evidence of the absent kidneys during development (Fig 1).

Fig 1: This posterior view of the organ block shows the large appearance of the flattened, pale adrenals in this 23 weeks of gestation infant with an intrapartum death. The vas deferens was also absent.
A kidney may be absent on only one side often with associated anomalies including absence of the ipsilateral side of the uterus and Fallopian tube (Fig 2).

Fig 2: There is an absent kidney and ipsilateral loss of the hemi-uterus and Fallopian tube. This 23 weeks of gestation infant was an intrapartum death, who also had anencephaly.
Fused kidneys (Horseshoe kidneys): The fusion of the kidneys usually occurs in the midline of the lower pole and they may be ectopic in that they are caudad in location. The anomaly is more common in Monosomy X (Turner syndrome). (Fig 3)

Fig 3: These kidneys fused at the lower pole were an incidental finding in this 23 weeks of gestation infant who died 2 hours prior to delivery following premature rupture of membranes and umbilical cord prolapse.
Ectopic kidneys: The position of the kidney can show abnormalities presumably from development and most commonly is near the pelvis. (Fig 4)

Fig 4: This is an ectopic kidney position with the right kidney lower than the left with a short ureter.
Small or enlarged kidney: As with all organs, the kidneys stripped of perirenal fat are weighed and compared to norms including the kidney to brain ratio. Massive congestion and hemorrhage can result in large kidneys as well as various form of renal cystic disease (Fig 5).

Fig 5: These large red kidneys, weight 37 grams, with a full bladder were the consequence of an acute twin transfusion from the living twin during the death this 30 weeks of gestation monochorionic twin with an approximately 24 hours of postmortem retention.
In other cases, developmental anomalies result in small kidneys. One factor that delays renal tubular development (renal tubular dysgenesis) produces loss of or decreased proximal tubule development (see supplement “A” below). If the kidneys are symmetric, they can be weighted together, but if asymmetrical, they need to be weighed separately. (Fig 6)

Fig 6: The right kidney was small 1.5 g compared to the left 2.0 g without histological difference. The infant was 22 weeks of gestation and had died 17 hours prior to delivery in a mother with severe early onset preeclampsia. The infant was small for gestation, 339 g, and the placenta had multiple infarctions and a 10% premature placental separation with underlying retroplacental hematoma.
Increased perirenal adipose tissue: With macrosomia in the infants of diabetic mothers, there is prominent subcutaneous adipose tissue, especially in the cheeks, but also over the pericardium, and kidney. (Fig 7)

Fig 7: This posterior organ block compares the intact perirenal fat to the right kidney from which the fat had been stripped. This is a 33 weeks of gestation infant of a diabetic mother with approximately 48 hours of postmortem retention.
Discolored kidney: Infarctions, umbilical vein thrombus, cystic disease or massive congestion/hemorrhage (Fig 5) can alter the color of the kidney making it pale or deeper red (Fig 8).

Fig 8: The kidney is pale with surface hemorrhages in this infant with unexplained oligohydramnios sequence in this 29 weeks of gestation infant with approximately 24 hours of postmortem retention.
Masses: The kidney may demonstrate Wilms tumor, congenital mesoblastic nephroma, or solitary cysts.
Dissection and sampling:
The renal vein is opened, and the ureters and renal artery are examined externally. The kidney is then removed and weighed. It can then be split longitudinally (bivalved) to reveal internal structure, particularly patterns of cystic disease and hemorrhage (Fig 9a-c).

Fig 9a: This bivalved kidney is distorted by macrocysts of variable size that obscure the expected underlying renal anatomy except for the calyces. There was no evidence of urinary tract obstruction in this 20 weeks of gestation infant with an intrapartum death.

Fig 9b: This bivalved kidney demonstrates enlarged calyces and early cystic dyplasia associated with hydronephrosis and ectopic pelvic kidneys in this 19 weeks of gestation intrapartum death who had early jugular lymphatic obstruction sequence and monosomy X (Turner syndrome).

Fig 9c: This bivalved kidney from an infant with autosomal recessive polycytsic disease that with close examination demonstrates the dilated collecting ducts filled with fine crystalized oxalic acid.
Histologic samples taken parallel to the cut surface or perpendicular to it in larger kidneys will best reveal generations of nephrons. Focal lesions can be sampled.
Oligohydramnios sequence (Potter syndrome):
Oligohydramnios is associated with an increased risk of stillbirth. A major cause of oligohydramnios is lack of urine production or obstructed urinary outflow. Intrinsic renal causes include autosomal recessive polycystic kidneys, and renal tubular dysplasia which require microscope diagnosis. While some multicystic dysplasia is intrinsic as in familial aplasia/dysplasia, often it is secondary to obstruction at some level of the urinary tract. In such cases, the entire urinary tract needs to be evaluated for the correct diagnosis. The normal diameter of the ureters appears wide for the size of the kidney, but this may be due to the need for a low resistance tube. Hydronephrosis does occur but the ureter will be clearly distended, and the calyces will also appear thickened. The insertion of the ureter into the bladder may be abnormal. In obstruction to the outflow proximal from the kidneys, the bladder will be hypoplastic, but urethral obstruction will usually demonstrate a large bladder. The latter may rupture into the abdomen or through the urachus to the umbilical cord. The bladder with possible urethral obstruction is best opened from the apex toward the urethra so that the obstruction (posterior urethral valves, atresia or outflow mass) can be visualized prior to cutting through it. Another useful technique that also works on hypoplastic bladders is to inject the bladder in situ with radiocontrast and take AP and lateral films (Fig 10).
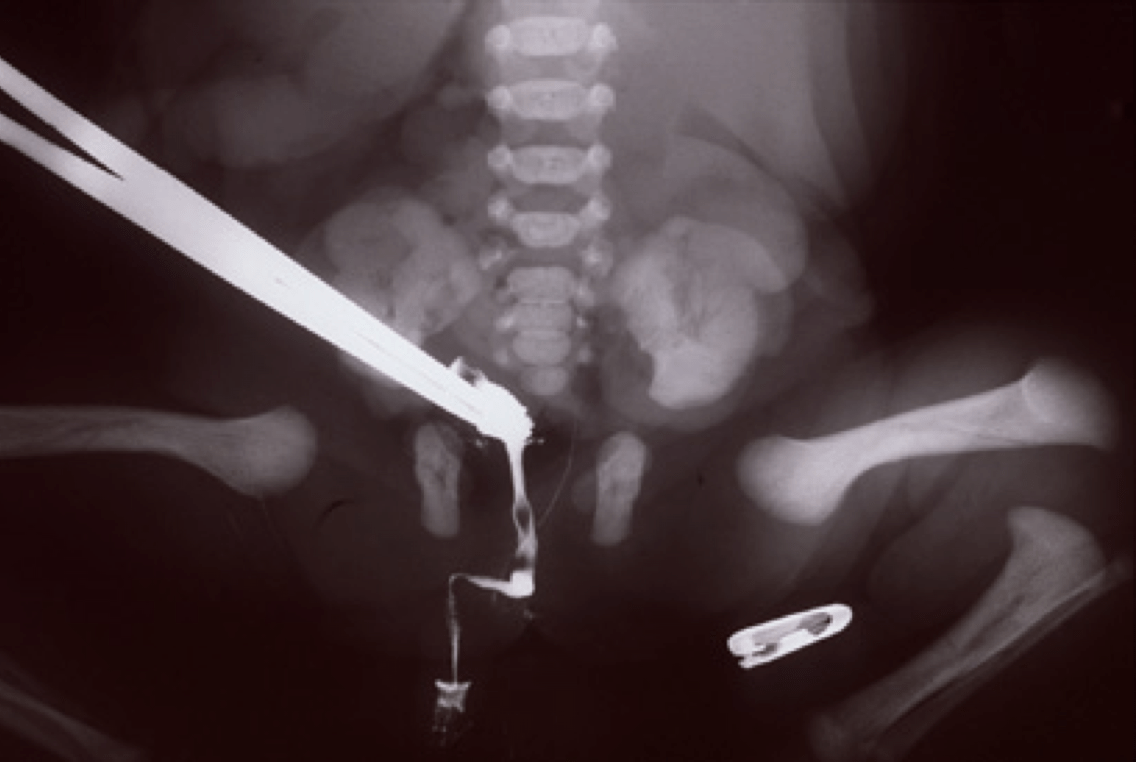
Fig 10: This is a postmortem cystogram of a hypoplastic bladder showing a patent urethra.
Potter sequence can also occur with prolonged rupture of fetal membranes or chronically decreased blood flow, as in chronic twin to twin transfusion. To develop the full oligohydramnios sequence (Potter facies, limb deformities, pulmonary hypoplasia, and amnion nodosum) requires almost complete anhydramnios, not just a decreased amount of fluid.
Microscopic Features:
Duration of postmortem retention: The loss of 1% of tubular basophilia occurs after 4 hours of postmortem retention and usually involves the straight and convoluted proximal tubules (Fig 11).

Fig 11: This image shows loss of nuclear basophilia primarily in straight and convoluted proximal tubules in this kidney from a 38 weeks of gestation infant with 24-48 hours of postmortem retention. The death was due to a 75% premature placental separation and underlying retroplacental hematoma. The ductus arteriosus showed evidence of constriction. (20x, H&E)
Complete loss of renal basophilia does not occur until 4 weeks of retention (Fig 12)

Fig 12: This image shows complete loss of basophilia in this 29 weeks of gestation infant with 3 weeks or more of postmortem retention. (20x, H&E)
Gestational age: The generations of nephrons branch in sequence from the urethral bud induction in the mesenchyme. Counting the generations had been proposed as a method of assessing gestational age. One simple extension of this is that after 35 weeks of gestation nephrogenesis ceases, and this is evidence of maturity [1, 2] (Fig 13 a,b).

Fig 13a: This kidney from a 28 weeks of gestation infant with approximately 12 hours of postmortem retention shows a basophilic rim of nephrogenesis along the outer cortical rim of kidney. (2x H&E)

Fig 13b: This kidney from a 40 weeks of gestation infant with 9 hours of postmortem retention shows some immature tubules and glomeruli but the rim of small blue cells of nephrogenesis is not present. (2x, H&E)
Renal vein thrombosis: The renal vein appears to be particularly susceptible in utero to thrombosis. This is most common in infants of diabetic mothers, but occurs in other thrombogenic circumstances as well (Fig 14a, b).

Fig 14a: The renal vein shows a laminated thrombus at the hilum with some calcification in this 37 weeks of gestation infant with 48 to 96 hours of intrauterine postmortem retention. The infant of a diabetic mother who demonstrated intrathoracic petechia. (H&E)

Fig 14b: The renal vein thrombus in this kidney from this 38 weeks of gestation infant of a diabetic mother demonstrates extensive calcification (48 to 96 hours of postmortem retention). (4x, H&E)
The basis for the localization of a thrombus in the renal vein in infants of a diabetic mother is unclear, but if glucosuria is part of the mechanism of polyhydramnios, it is possible that the blood leaving the kidney has had serum extracted to the point of being polycythemic and hyperviscous.
Congestion and hemorrhage: The kidney can show passive congestion in heart failure as in other organs, and occasionally hemorrhage. The congestion is often confined to the cortico- medullary junction, likely due to the shunting of arterial blood away from the cortex in asphyxia (15a, b).

Fig 15a: This kidney demonstrates venous congestion primarily at the corticomedullary junction in this 34 weeks of gestation infant with 2 hours of postmortem retention who suffered a large premature placental separation. (2x, H&E)

Fig 15b: This kidney demonstrates more extensive congestion and hemorrhage not only in the cortico-medullary area but also in the subcapsular cortex. The infant was 40 weeks of gestation with approximately 12 hours of postmortem retention following a large premature placental separation. (2x, H&E)
Hemorrhages can also occur with septic shock and presumed disseminated intravascular coagulation (Fig 15c).

Fig 15c: The extensive cortical hemorrhage in this infant was part of many visceral hemorrhages in this 29 week gestation infant with approximately 12 hours of postmortem retention with fetal sepsis with overgrowth of gram negative cocci, purulent chorioamnionitis and subacute necrotizing funisitis. (10x, H&E)
Mineralization within renal tubules: In some infants there are mineralized deposits of calcium and iron in the tubules. The most logical explanation is that these are residual hemorrhagic casts from a prior episode of acute tubular necrosis (Fig 16a-c).

Fig 16a: The dark mineralized deposits often tear the tissue, but their localization within the tubules can be seen focally (arrows). This 19 weeks of gestation infant with approximately 24 hours of postmortem retention was from a mother with sickle cell disease and one hospitalization for transfusion. (20x, H&E)

Fig 16b: This is the same kidney as Fig 16a. The mineralized casts stain positively for calcium. (20x, Von Kossa)

Fig 16c: This is the same kidney as Fig 16a. The mineralized casts stain positively for iron. (20x iron)
Renal cystic disease:
Cystic Dysplasia (Fig 17)
 Fig 17: This kidney shows many variable sized cortical cysts with little normal renal tissue. The diagnostic feature for multicystic dysplasia is the primitive ureteral ducts surrounded by basophilic connective tissue (arrows). Chondroid tissue may also be present. There was no evidence of urinary tract obstruction. The infant was an intrapartum death at 20 weeks of gestation to a diabetic mother. (2x, H&E)
Fig 17: This kidney shows many variable sized cortical cysts with little normal renal tissue. The diagnostic feature for multicystic dysplasia is the primitive ureteral ducts surrounded by basophilic connective tissue (arrows). Chondroid tissue may also be present. There was no evidence of urinary tract obstruction. The infant was an intrapartum death at 20 weeks of gestation to a diabetic mother. (2x, H&E)
Autosomal Recessive polycystic disease (Fig 18)
 Fig 18: This kidney shows the ectactic collecting ducts typical of autosomal recessive polycytic kidney disease or in this case in short rib polydactyly in a 32 weeks of gestation infant with 2 days of survival. (10x, H&E)
Fig 18: This kidney shows the ectactic collecting ducts typical of autosomal recessive polycytic kidney disease or in this case in short rib polydactyly in a 32 weeks of gestation infant with 2 days of survival. (10x, H&E)
Glomerulocystic disease (Fig 19)
 Fig 19: This kidney demonstrates glomerular cystic disease as part of complex malformation syndrome. The arrows point to the glomerular tufts protruding into the cyst. The infant was 32 weeks of gestation and survived 1 hour. (4x, H&E)
Fig 19: This kidney demonstrates glomerular cystic disease as part of complex malformation syndrome. The arrows point to the glomerular tufts protruding into the cyst. The infant was 32 weeks of gestation and survived 1 hour. (4x, H&E)
Infection: The renal tubules are a common target of congenital CMV infection (Fig 20).
 Fig 20: The center of the image shows several cells in one tubule with prominent cytomegalovirus inclusions. This is from a 21 weeks of gestation infant with 1 hour of survival. (40x, H&E)
Fig 20: The center of the image shows several cells in one tubule with prominent cytomegalovirus inclusions. This is from a 21 weeks of gestation infant with 1 hour of survival. (40x, H&E)
Toxoplasma cysts may be trapped in glomeruli (fig 21).
 Fig 21: The kidney shows a toxoplasmosis cyst trapped in the renal glomerulus in this 21 weeks of gestation infant with 24 to 48 hours of postmortem retention. (100x, H&E)
Fig 21: The kidney shows a toxoplasmosis cyst trapped in the renal glomerulus in this 21 weeks of gestation infant with 24 to 48 hours of postmortem retention. (100x, H&E)
Extramedullary hematopoiesis: (Fig 22)
 Fig 22: This image from the perihilar area of the kidney demonstrates extensive extramedullary hematopoiesis(EMH). This is from the same infant in Fig 20 who had hepatospenomegaly and skin lesions from EMH. (20x, H&E)
Fig 22: This image from the perihilar area of the kidney demonstrates extensive extramedullary hematopoiesis(EMH). This is from the same infant in Fig 20 who had hepatospenomegaly and skin lesions from EMH. (20x, H&E)
References:
1. Potter, E. and T. ST, Glomerular development in the kidney as an index of fetal maturity. J Pediatr, 1943. 22: p. 695-706.
2. Fujikura, T. and L. Froehlich, Birthweight, gestational age, and renal glomerular development as indices of fetal maturity. Am J Obstet Gynecol, 1972. 113: p. 627-631.
3. Allanson, J.E., J.T. Pantzar, and P.M. MacLeod, Possible new autosomal recessive syndrome with unusual renal histopathological changes. Am J Med Genet, 1983. 16(1): p. 57-60.
4. Voland, J.R., et al., Congenital hypernephronic nephromegaly with tubular dysgenesis: a distinctive inherited renal anomaly. Pediatr Pathol, 1985. 4(3-4): p. 231-45.
5. Landing, B.H., et al., Labeled lectin studies of renal tubular dysgenesis and renal tubular atrophy of postnatal renal ischemia and end-stage kidney disease. Pediatr Pathol, 1994. 14(1): p. 87-99.
6. Schwartz, B.R., et al., Isolated congenital renal tubular immaturity in siblings. Hum Pathol, 1986. 17(12): p. 1259-63.
7. Bernstein, J., Renal tubular dysgenesis. Pediatr Pathol, 1988. 8(4): p. 453-6.
8. Swinford, A.E., et al., Renal tubular dysgenesis: delayed onset of oligohydramnios. Am J Med Genet, 1989. 32(1): p. 127-32.
9. Cunniff, C., et al., Oligohydramnios sequence and renal tubular malformation associated with maternal enalapril use. Am J Obstet Gynecol, 1990. 162(1): p. 187-9.
10. Genest, D. and J. Lage, Absence of normal-appearing proximal tubules in the fetal and neonatal kidney: prevalence and significance. Hum Pathol, 1991. 22: p. 147-153.
11. Barr, M.J. and M.M.J. Cohen, ACE inhibitor fetopathy and hypocalvaria: the kidney-skull connection. Teratol, 1991. 44: p. 485-495.
12. Martin, R., et al., Effect of ACE inhibition on the fetal kidney: decreased renal blood flow. Teratol, 1992. 46: p. 317-321.
13. Allanson, J.E., et al., Renal tubular dysgenesis: a not uncommon autosomal recessive syndrome: a review [see comments]. Am J Med Genet, 1992. 43(5): p. 811-4.
14. Metzman, R.A., M.A. Husson, and E.A. Dellers, Renal tubular dysgenesis: a description of early renal maldevelopment in siblings. Pediatr Pathol, 1993. 13(2): p. 239-48.
15. Pryde, P.G., et al., Angiotensin-converting enzyme inhibitor fetopathy. J Am Soc Nephrol, 1993. 3(9): p. 1575-82.
16. Bernstein, J. and L. Barajas, Renal tubular dysgenesis: evidence of abnormality in the renin- angiotensin system.J Am Soc Nephrol, 1994. 5(2): p. 224-7.
17. Moldavsky, M., A. Shahin, and H. Turani, Renal tubular dysgenesis present in a newborn with meconium ileus.Pediatr Pathol, 1994. 14(2): p. 245-51.
18. Jain, V. and D. Beneck, Renal tubular dysgenesis in an hydropic fetus with trisomy 21: a case report with literature review. Pediatr Dev Pathol, 2003. 6(6): p. 568-72.
19. postrenal., S.n.t.t.p.r.









