Duration of Postmortem Retention
Amanda Saunders, MD, MBA & Robert Bendon, MD
(All photos are submitted courtesy Dr. Robert Bendon MD, unless otherwise specified)
A. Introduction
The infant in utero is in a relatively constant temperature, often aseptic, environment and there are often no internal microbial flora to cause putrefaction. Fetal death, under these conditions, results in a progressive cellular autolysis at a predictable rate. Activation of lysozymes is manifested as tissue softening and loss of nuclear basophilia. Failure of the ATP pump and cell membrane integrity results in discoloration from the diffusion of hemoglobin. These intrauterine postmortem changes are often referred to as maceration, a reference to softening in a liquid. With delivery, primarily due to cooling and a dry environment, the maceration is effectively stopped. The ordered progression of changes encouraged pathologists to estimate how long the infant had been dead in utero. Early studies relied on decreased fetal movement, or loss of auscultated fetal heart tones to determine the time of fetal death [4-6]. In retrospect, this gave a false estimate of the timing.
Genest and colleagues solved the problem in a study in which they identified a subset of stillborn infants for which an interval could be determined between the last ultrasound or Doppler evidence of fetal life and similar evidence of fetal death [1-3]. Thus, an infant could be classified as having died within an interval, for example between 12 (last evidence alive) to 24 hours (first evidence of death) prior to birth. Specific features determined from gross photographs, and from microscope slides of the autopsy and placenta, were then used to statistically predict the interval of death, and the best predictors were confirmed in a blinded study. Using the results of this study, an estimate of the duration of intrauterine post mortem retention should be included in the evaluation of the autopsy of stillborn infants.
The postmortem intrauterine retention interval is important in relating the mechanism of death to underlying events. For example if a retroplacental hemorrhage is very acute, but the infant has been dead for more than 48 hours, then clearly abruption was not the cause of the death. The pathologist must be as accurate as possible in determining the retention interval and aware that the estimate may be in error, although in the Genest studies usually by only a single interval. The implication for an infant retention of less than 24 hours with decreased fetal movement for three days is that an opportunity for intervention was missed.
B. Clinical timing of death
As implied by the Genest studies, the clinical chart can be helpful in bracketing the time of death using the last time there was ultrasound or Doppler evidence of fetal heart tones, the first time there was evidence of fetal death, and the time of delivery. The mother’s recollection of last normal fetal movements, and when she first noted cessation of movement are important to correlate with anatomic information. In some cases the time of death is known to be intrapartum, or even occurs under observation. Additional information that may be important is a history of trauma, or a history of violent fetal movements prior to cessation of movements. Collin’s has suggested that an excess of fetal deaths, based on loss of fetal movement, occur during the night possibly related to maternal hypercapnia (fetal acidosis and a gradual mechanism of death)[7].
C. External features:
1. The umbilical cord:
With death, the hemoglobin in the umbilical cord vessels diffuses into the surrounding Wharton’s jelly. The arteries typically are not constricted, as they would be in a liveborn infant. There are exceptions with constricted umbilical arteries in very recent or intrapartum stillbirth. Hemoglobin can stain from all three vessels, not just the vein. The cord may show no staining, partial staining or complete staining. Staining of the umbilical cord by old meconium or blood in the amnion can be excluded by finding similar staining of the fetal membranes. The extension of staining from the umbilical vein into an otherwise white or gray Wharton’s jelly occurs earlier than complete staining of the cord. With time the red hemoglobin breaks down into pigments giving a brown cast.
A striking example in which staining of the umbilical cord is not from postmortem retention occurs with a thrombus of the umbilical artery which is not lethal as long as there are two such arteries (Fig 1).

An occlusive umbilical artery thrombus stops blood flow in the entire artery, leaving the red cells in essentially the same condition of stasis that occurs with fetal death. Diffusion of oxygen from the flow in the other artery and the vein do not appear to keep the red cells viable. The red cell hemoglobin will diffuse from the artery forming a candy stripe helix that follows the vessel. This could give a false impression of longer postmortem retention, yet in many cases the infant is live born. Another cause of potential error is fetal anemia or exsanguination that may cause the cord to appear unstained or only pale stained despite other evidence of prolonged retention
In the Genest study, brown or red-brown discoloration of the umbilical cord was evaluated[2]. Brown or red staining initially appeared to be a good predictor of ≥ 6 hours retention, but in the blinded study was not as powerful.
The umbilical cord may be overly twisted and may be tightly twisted and thinned at the umbilicus. This can be a post mortem event related to passive motion causing spinning of the fetus in the amniotic fluid. This twisting is often a finding in midtrimester fetuses with very prolonged post mortem intrauterine retention. The topics of fetal umbilical constriction, thrombosis and torsion will be considered in more detail in other sections.
2. Color of the sclera:
Like the umbilical cord, the sclera provides a white background and a limited number of vessels (although smaller) for evaluating the diffusion of hemoglobin. The feature was not evaluated by Genest and Singer [2].
3. Overlapping of skull bones:
As the tissue undergoes autodigestion, the connective tissue weakens, and the cranial bones may overlap. This feature was utilized in obstetrics prior to ultrasound, because it could be demonstrated by radiograph. Described by Spalding, it was definitive evidence of fetal demise [8]. This feature correlates with softening of the brain and a loss of adhesion of the skull bones to the dura.
4. Skin color:
Skin color does not refer to the melanin content of the epidermis, but to diffusion of hemoglobin from small vessels in the dermis, and the breakdown of hemoglobin changing from red to brown to pale tan. The changing color from normal pink, partial red, totally red, at least partially brown to at least partially tan were evaluated by Genest and Singer [2]. Initially brown or tan skin color was a good predictor of ≥ 24 hours retention, but did not retain this power in the blinded study. Skin color may not show color changes if there is fetal anemia, blood loss or peripheral vasoconstriction.
5. Turgor of the eyes:
In the third trimester a sunken ocular globe appears to associate with other features of prolonged retention such as liquefaction of the brain.
6. Flexibility of the joints:
The joints become hyperextensible assuming unnatural positions with prolonged postmortem retention. Fixed deformations appear to be maintained, but some deformations may occur from post mortem positioning especially with oligohydramnios. There is not good information about the reliability of limb deformation with prolonged retention. The significance of limb findings may be clarified by correlation with other features of retention and the clinical history. A potentially confounding finding is the hyperflexibility of the limbs in Larson syndrome. These infants may die intrapartum presumably due to the laxity of the atlanto-occiptal joint.
7. Desquamation and bullae of the skin:
With post mortem retention, the epidermis separates from the dermis. If the edges of areas of desquamated skin remain attached, fluid may accumulate forming a bulla. In areas where the desquamation is lifted, bare patches of dermis are exposed. While some of these patches may occur spontaneously, pressure can produce them even with post mortem handling. In infants with short retention intervals, gentle pressure may produce desquamation, even though there was none present on initial examination. Aside from subtle darkening of the mucus membranes, this phenomenon may be the only anatomic evidence that the death was intrauterine.
Genest and Singer evaluated many features of desquamation, and found several to be good predictors of the retention interval [2]. An area of desquamation ≥ 1 cm predicted greater than 6 hours retention. Desquamation of the face, back or abdomen predicted a retention of ≥ 12hours. Desquamation of ≥ 5% of the body or involving 2 or more zones (scalp, face, neck, chest, abdomen, back, arms, hand, leg, foot or scrotum) predicted ≥ 18 hours of retention. Thus, even with the potential of artifact, the description of desquamation may still be a useful measure of retention, but causes of artifact should still be considered, such as a difficult delivery, or prolonged handling of the body.
The separation is at the epidermal dermal junction. A potential cause of error is that epidermolysis bullosae may occur in utero, and even with an intra or post partum death, and would have advanced desquamation. Other features of prolonged retention should be absent. [9, 10].
8. Mummification:
These fetuses resemble the desiccation of mummies and have a pale tan color. They are usually compressed as well. This feature is commonly seen with the fetus papyraceusin which one twin dies mid-trimester and the pregnancy continues until the third trimester. Mummification proved to a good predictor of ≥ 2 weeks of retention [2].
D. Internal features:
1. Consistency of the brain:
The brain progressively softens with retention, and also shows increasing hemoglobin staining. At the earliest stage the brain can be removed normally and remains intact, this progresses to a semisolid stage in which the cerebrum can often still be removed with a portion intact, to an end stage in which the brain is liquid.
2. Color of the viscera:
The viscera have distinct colors in death without retention. These colors fade and eventually most of the viscera take on a similar muddy and then tan color. The changes follow the diffusion and breakdown of hemoglobin generally. Consequently, fluid in cavities also discolors from the hemoglobin. This should not be mistaken for blood stained fluid. With prolonged retention, petechiae on surfaces may become imperceptible, although they may still be identifiable microscopically from the red cell membranes.
3. Softness of the viscera:
Visceral organs soften with retention, and this should not be mistaken for pathology. The liver may be so soft that with delivery of the very preterm fetus it may rupture into a liquid paste in the abdomen. In vertex delivery, the liquid brain may be extruded into body cavities mimicking a tumor [11]. Conversely, a tumor may become a paste in the abdomen, only identified by the absence of the involved organ, usually adrenal or kidney. In first trimester cases with prolonged retention, fixation of the fetus prior to dissection may prevent organ damage during dissection that could compromise diagnosis.
E. Placental examination:
The placental histology may provide some objective evidence of the retention interval in stillborn infants who are not autopsied. The villi are maintained by the maternal circulation (although the flow decreases) but the fetal circulation ceases with death. This causes a sequence of change starting with karyorhexsis of nucleated fetal blood cells. This is followed by proliferation of endothelial cells into the lumen of larger vessels, obliteration of smaller vessels, and villous stromal fibrosis. To be valid as a measure of postmortem retention duration, these changes should be diffuse in the placenta. Fetal thrombotic vasculopathy can cause stasis in fetal vessels with focal changes similar to those caused by fetal death.
Genest evaluated placental histology and found only three high predictor features, which defined only 4 intervals, < 6hrs, 6 hours to 48 hours, 48 hours to 14 days, and more than 14 days [1]. Intravascular karyorrhexis estimated ≥ 6 hrs of retention, stem vessel luminal abnormalities whether endothelial or obliterative correlated with ≥ 48 hours if present in 10-25 % of villi and with ≥ days if more than25 % of villi involved. Extensive villous fibrosis was also correlated with ≥ 14 days. In a study of placentas from terminated second trimester fetuses (18-23 weeks of gestation) with 4 intervals of postmortem retention (<12 hours, 12-24 hours, 24-36 hours, and >36 hours, neither intravascular karyorrhexis nor changes in blood lumen were statistically valid predictors of the duration of fetal retention[12]. Degeneration of umbilical vascular smooth muscle was present in only 33% of the <12 hour duration, and 100% in the longer durations.
F. Estimate of retention from the microscopic slides
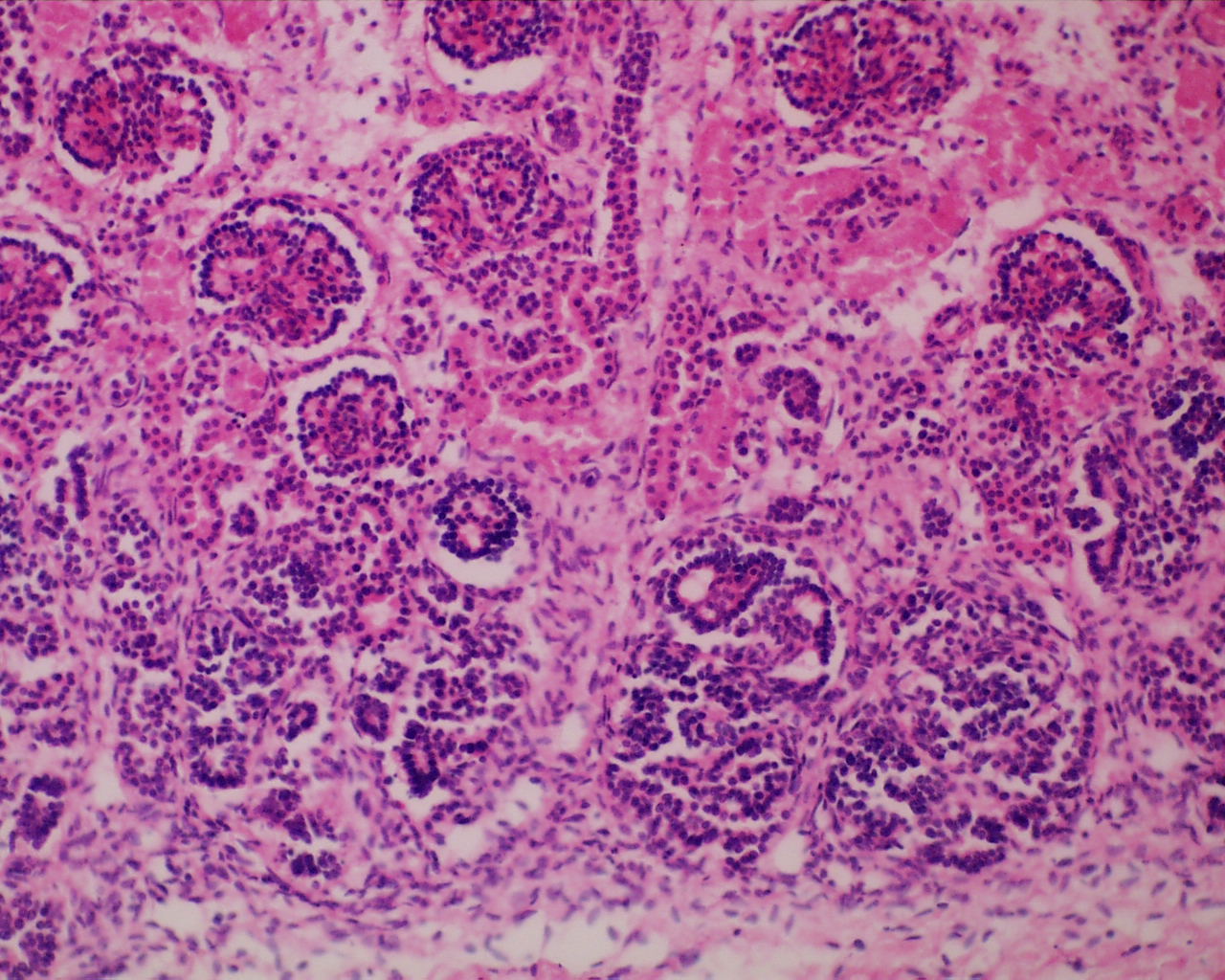
In some ways death is like an infarction in that hypoxia will lead cells to eventually become acidotic releasing digestive enzymes from lysomes. Unlike death in the usual external environment, the fetus remains at body temperature, the idea temperature for these lysosomal enzymes to digest cell proteins and nucleic acids. The rate or onset of this autodigestion appears to vary with each organ. The Genest studies found that the best measure of postmortem retention interval was the loss of basophilia in nuclei of different tissues [3]. Loss of basophilia was defined as at least 1% of nuclei entirely devoid of basophilic staining (Fig 2).

Fig 2 Renal tubules showing greater than 1% loss of nuclear basophilia.
G. Forensic Complications:
A common forensic problem is determining if an abandoned, deceased infant was a livebirth or a stillborn. Evidence of in utero postmortem retention is evidence of stillbirth. Natural conditions may result in autolysis that can make problematic the evaluation of the features used in the Genest studies, for example infants found after unknown periods in a plastic bag in a warm trash bin. Desquamation with bullae is usually reliable evidence of post mortem retention in infants in dry conditions, but factors mimicking changes of retention after delivery are not completely studied. Focal expansion of the airways is also not reliable evidence of livebirth. A constant observation in stillborn infant placentas is that the umbilical arteries are consistently dilated. In live born infants the arteries constrict, although focally they will be dilated where blood has been trapped by the constriction. A logical evaluation of all the evidence keeping in mind the limitations of the scientific knowledge is necessary in some cases to determine if there was a livebirth.
References
- Genest, D.R., Estimating the time of death in stillborn fetuses: II Histologic evaluation of the placenta: a study of 71 stillborns.Obstet Gynecol, 1992.80: p. 585-592.
- Genest, D.R. and D.B. Singer, Estimating the time of death in stillborn fetuses: III. External fetal examination; a study of 86 stillborns.Obstet Gynecol, 1992. 80(4): p. 593-600.
- Genest, D.R., M.A. Williams, and M.F. Greene, Estimating the time of death in stillborn fetuses: I. Histologic evaluation of fetal organs; an autopsy study of 150 stillborns.Obstet Gynecol, 1992. 80: p. 575-84.
- Thomson, C., The pathology of foetal maceration.J Obstetr Gynaecol Brit Empire, 1927. 34: p. 40-71.
- Ballantyne, J., Ante-natal, intra-natal, and neo-natal death: Causes, pathology and prevention with special reference to ante-natal death.Brit Med J, 1922. 2: p. 583-588.
- Strachan, G.I., The pathology of foetal maceration A study of 24 cases.Br Med J, 1922. 2: p. 80-2.
- Collins, J.H., Umbilical cord accidents–time of death?Am J Obstet Gynecol, 1997. 177(6): p. 1566.
- Spalding, A.B., Surg Gynecol Obstet 1922. 34: p. 754-757.
- Azarian, M., et al., Prenatal diagnosis of inherited epidermolysis bullosa in a patient with no family history: a case report and literature review.Prenat Diagn, 2006. 26(1): p. 57-9.
- Lepinard, C., et al., Prenatal diagnosis of pyloric atresia-junctional epidermolysis bullosa syndrome in a fetus not known to be at risk.Prenat Diagn, 2000. 20(1): p. 70-5.
- van Noort, G. and A. de la Fuente, So-called primitive neuroectodermal tumor in macerated fetuses: A confusing artifact.Pediatr Pathol, 1988. 8: p. 359-365.
- Jacques, S.M., et al., Estimation of time of fetal death in the second trimester by placental histopathological examination.Pediatr Dev Pathol, 2003. 6(3): p. 226-32.









