
Authors: Meagan Chambers MD, Amanda Saunders MD MBA, Alex Williamson MD
Background
SARS‐CoV‐2 (severe acute respiratory syndrome corona virus 2), the virus that causes COVID‐19 (coronavirus disease 2019), first appeared as a novel coronavirus in fall
- It is similar to the severe acute respiratory syndrome coronavirus (SARS‐CoV‐1) in that both viruses share similar clinical presentations, peak viral loads in lower respiratory samples, and a common cellular entry receptor (angiotensin converting enzyme 2 [ACE2]). However, the viruses are distinct in many ways, and the novel SARS‐CoV‐2 virus has been responsible for a global pandemic with far‐reaching health, social, and economic consequences.
The goal of the autopsy pathologist in evaluating potential COVID-19 deaths is to
1) Document findings associated with COVID-19
2) Assess efficacy and status of medical/therapeutic interventions
3) Document pre-existing conditions which are known to increase the mortality rate of COVID-19. These include (but are not limited to)
- Hypertensive cardiovascular disease
- Atherosclerotic cardiovascular disease
- Diabetes mellitus
- Obesity
- Preexisting respiratory disease (e.g. COPD)
 Image: Figure comparing pre-existing conditions in study on decedents with COVID-19 in 2020 compared to follow up study in 2022 (Figure Credit: Hooper 2024).
Image: Figure comparing pre-existing conditions in study on decedents with COVID-19 in 2020 compared to follow up study in 2022 (Figure Credit: Hooper 2024).
Quick Tips at Time of Autopsy
Clinical History
- A positive postmortem nasopharyngeal swab or other diagnostic test is frequently present in the patient’s clinical history. Occasionally, SARS-CoV-2 will be detected on postmortem nasopharyngeal swab.
- Vaccine status (vaccine type, administration date, boosters, etc.)
- If available in the record, making note of the pathologic variant (e.g. alpha, beta, delta, omicron, etc.) can be useful for epidemiologic purposes including vaccine efficacy.
- Clinical comorbidities that increase mortality (as mentioned above)
- Hospitalization and ventilation duration (which has an effect on pulmonary pathology)
- In pediatric patients post-acute sequelae of COVID-19 (a post-inflammatory, Kawasaki-like syndrome) can be seen although there are no characteristic pathologic features at autopsy. The diagnosis could be in the differential for a pediatric case.
 Image: Table comparing demographics of descents with COVID-19 in 2020 vs follow up study in 2022 (Figure Credit: Hooper 2024).
Image: Table comparing demographics of descents with COVID-19 in 2020 vs follow up study in 2022 (Figure Credit: Hooper 2024).
External examination
Devices that may be present:
- Endotracheal tube
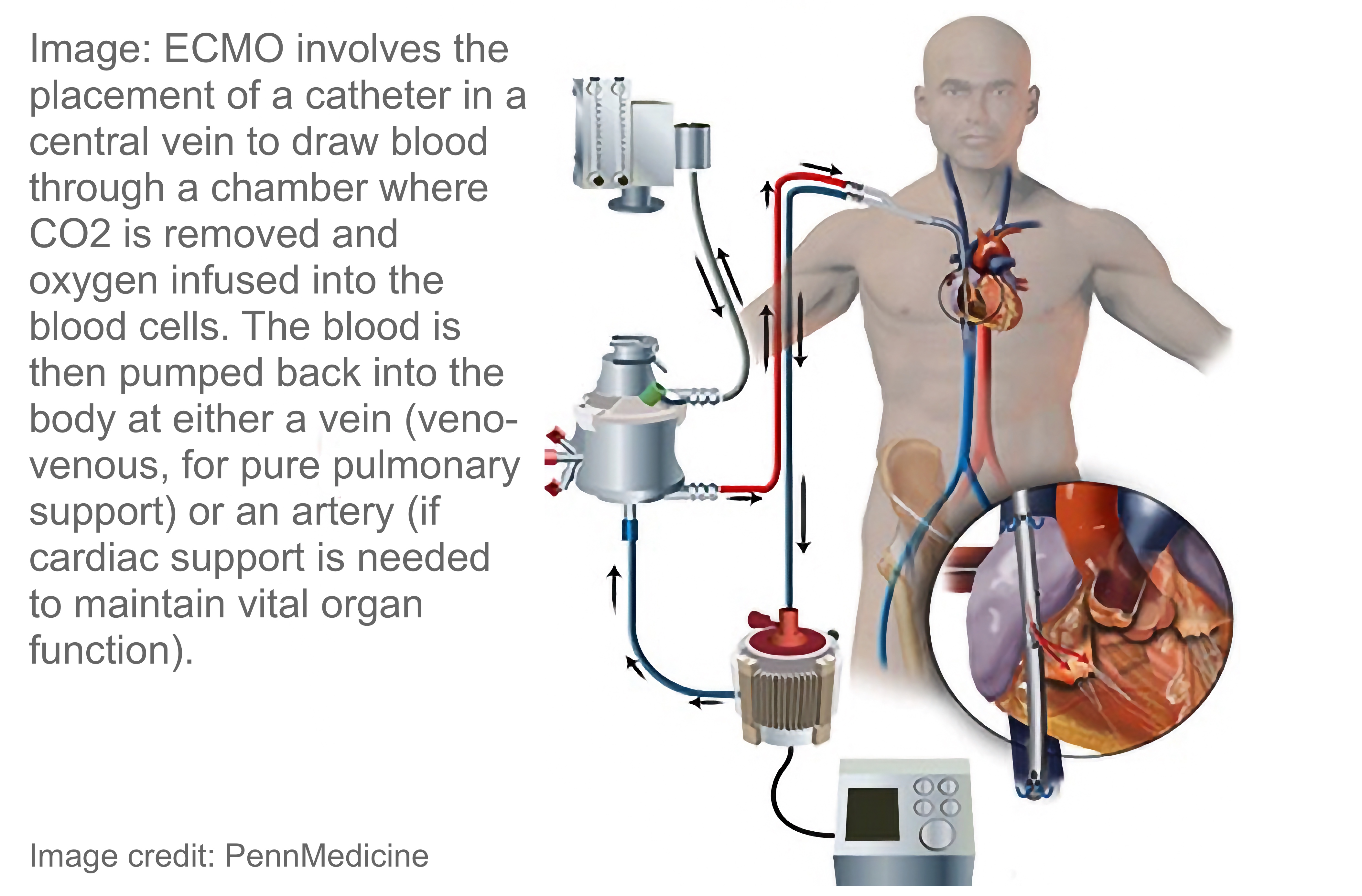
- Extracorporal membranous oxygenation (ECMO)

Internal examination
- Devices (as above) – including internal placement
Lungs:
- Heavy lungs (each over 1000 g) with red/tan and mottled surfaces and with a variable amount and distribution of consolidation (i.e. fluid, cells, and/or other material filling affected air spaces) including edema and/or hemorrhage.
- Areas of atelectasis, airways containing viscous mucus, and/or pleural effusions may be present.
- Pulmonary thromboemboli may be present in large or small vessels; larger emboli may be associated with pulmonary infarcts (see the Pulmonary Thromboemboli article).
- Deep leg vein dissection should be undertaken in cases where antemortem or postmortem evidence of pulmonary thromboemboli are present.
Ancillary Testing
- Postmortem nasopharyngeal swab if antemortem nasopharyngeal swab is not available or was remote (e.g. >7 days).
- Postmortem cultures (per usual practice; see the postmortem cultures article for more information).
Quick Tips at Time of Histology Evaluation
Lungs
- Diffuse alveolar damage (DAD) in the acute and/or organizing phases is the hallmark of COVID-19
- 1-7 days: The exudative (acute) phase of DAD. Characterized by neutrophilic inflammation, intra-alveolar hemorrhage, edema, and hyaline membranes
- 1-3 weeks: The Proliferative (subacute) phase. Characterized by proliferation of myofibroblasts (leading to interstitial inflammation and fibrosis) and decreased edema due to type II pneumocyte regeneration
- >3 weeks: Fibrotic (chronic) phase. Characterized by collagenous fibrosis in alveolar and interstitial spaces and refractory rigidity of alveoli due to architectural remodeling.
- The presence of acute (exudative) vs organizing DAD commonly correlates with the duration of symptoms; however, features of organizing DAD can occur in patients with rapidly progressive fatal COVID-19.
- Similarly, fibrosis can be quite extensive in patients within only a few weeks.
The presence of an organizing fibrous process in the lungs can be due to DAD secondary to SARS‐CoV‐2 pneumonitis and/or ventilator-induced lung injury.
 Image: Schematic representation of the time course of the acute respiratory distress syndrome (ARDS). During the early (or exudative) phase, the lesion is characterized by high permeability pulmonary edema followed by the formation of hyaline membranes. After seven to ten days, a proliferative phase may develop, with marked interstitial inflammation, fibrosis, and disordered healing. (Image credit: UpToDate-ARDS).
Image: Schematic representation of the time course of the acute respiratory distress syndrome (ARDS). During the early (or exudative) phase, the lesion is characterized by high permeability pulmonary edema followed by the formation of hyaline membranes. After seven to ten days, a proliferative phase may develop, with marked interstitial inflammation, fibrosis, and disordered healing. (Image credit: UpToDate-ARDS).
 Image: Acute diffuse alveolar damage (DAD) with hyaline membranes lining air spaces (arrows), H&E 10x. (Image credit: Meagan Chambers, University of Washington).
Image: Acute diffuse alveolar damage (DAD) with hyaline membranes lining air spaces (arrows), H&E 10x. (Image credit: Meagan Chambers, University of Washington).
 Image: Organizing diffuse alveolar damage (DAD) with loss of airspaces and a near confluent mix of hyaline membrane/fibrin deposition, fibroblasts, and debris; H&E’s 4x (left) and 10x (right). (Image credit: Meagan Chambers, University of Washington).
Image: Organizing diffuse alveolar damage (DAD) with loss of airspaces and a near confluent mix of hyaline membrane/fibrin deposition, fibroblasts, and debris; H&E’s 4x (left) and 10x (right). (Image credit: Meagan Chambers, University of Washington).
 Image: A composite H&E (left) and trichrome (right) of DAD in the fibroproliferative stage. Note the diffuse trichrome staining highlighting the interstitial and airway fibrosis in blue. (Image credit: Meagan Chambers/Stanford University).
Image: A composite H&E (left) and trichrome (right) of DAD in the fibroproliferative stage. Note the diffuse trichrome staining highlighting the interstitial and airway fibrosis in blue. (Image credit: Meagan Chambers/Stanford University).
 Image: Resolving DAD may appear as clear airspaces with residual hyaline membranes/wall remodeling (arrows) as well as large airspaces which do not completely heal. (Image: Meagan Chambers/Stanford University).
Image: Resolving DAD may appear as clear airspaces with residual hyaline membranes/wall remodeling (arrows) as well as large airspaces which do not completely heal. (Image: Meagan Chambers/Stanford University).
Chronic interstitial inflammation can be present in a patchy distribution with variably prominent perivascular lymphocytic infiltrate is also observed, although this pathology is relatively uncommon.
- The presence of bronchopneumonia and/or foci of neutrophilic inflammation is concerning for a superimposed bacterial infection and is not a typical feature of COVID-19.
- Acute fibrinous and organizing pneumonia (AFOP), with its characteristic pattern of fibrosis and intra‐alveolar fibrin balls, can occur in addition to DAD, and rarely can represent the predominant pattern of parenchymal injury in COVID‐19.
- Pulmonary thrombosis can be a feature of DAD and therefore can be seen in COVID-19; thrombi can form in the site of tissue injury (thrombus) or travel to the lungs (thromboemboli). Differentiating thrombi and thromboemboli in the lungs requires correlation with other autopsy findings (e.g. presence of deep vein thrombosis, large or macroscopic thromboemboli).
- Although not required for diagnosis, IHC for SARS‐CoV‐2 can be performed at some reference laboratories and if desired.
 Image: Positive immunohistochemistry for SARS-CoV-2 in lung tissue. (Image credit: Meagan Chambers, University of Washington).
Image: Positive immunohistochemistry for SARS-CoV-2 in lung tissue. (Image credit: Meagan Chambers, University of Washington).
Peripheral vasculature
- Evaluate and approximately date thrombi in deep veins including the lower extremities.
 Table: Pulmonary peripheral vasculature findings in a large series of COVID-19 autopsies. These reflect a combination of pathologies intrinsic to COVID-19 and pathologies from preexisting conditions (Table credit: Hooper 2021).
Table: Pulmonary peripheral vasculature findings in a large series of COVID-19 autopsies. These reflect a combination of pathologies intrinsic to COVID-19 and pathologies from preexisting conditions (Table credit: Hooper 2021).
Heart
- Pre-existing conditions are the most salient findings in the heart.
- Myocarditis is not a salient feature of COVID-19; in systematic reviews and multi‐institutional studies, the overall prevalence of myocarditis is low (2%‐6%).
- Rare cardiac complications of COVID-19 can also include acute ischemic myocardial injury (<10%), pericardial effusion (<3%), and/or endocardial thrombi (<5%).
 Table: Cardiac findings in a large series of COVID-19 autopsies. These reflect a combination of pathologies intrinsic to COVID-19 and pathologies from preexisting conditions (Table credit: Hooper 2021).
Table: Cardiac findings in a large series of COVID-19 autopsies. These reflect a combination of pathologies intrinsic to COVID-19 and pathologies from preexisting conditions (Table credit: Hooper 2021).
Kidney
- Pre-existing conditions are the most salient findings in the kidney.
- Acute tubular injury is common and probably reflects hypoxic ischemic injury secondary to lung pathology (as above).
- Microthrombi in glomerular capillaries are rare and can reflect either hypercoagulability in the setting of COVID-19 and/or disseminated intravascular coagulation (DIC)/shock.

Table: Renal and hepatic findings in a large series of COVID-19 autopsies. These reflect a combination of pathologies intrinsic to COVID-19, secondary to shock/multisystem organ dysfunction, and pathologies from preexisting conditions (Table credit: Hooper 2021).
Brain:
- Microglial nodules are a non-specific feature of viral illnesses which can also be seen in some cases of COVID-19.
Pre-existing conditions:
- Cardiovascular comorbidities, especially hypertension and coronary artery disease, are among the most prominent preexisting conditions linked to increased severity and mortality in COVID‐19.
- Histologic evidence of comorbidities/pre-existing conditions should be documented.
- Hypertensive cardiovascular disease (e.g. myocyte hypertrophy, interstitial myocardial fibrosis, nephroarteriosclerosis)
- Atherosclerotic cardiovascular disease (e.g. replacement myocardial fibrosis)
- Diabetes mellitus (e.g. nodular mesangial glomerular sclerosis/Kimmelstiel-Wilson lesions, nephroarteriosclerosis)
- Preexisting respiratory disease (e.g. emphysema, asthma)
- Obesity (e.g. hepatic steatohepatitis)
Quick Tips at Time of Reporting
- Document typical pathologies of COVID-19 (e.g. DAD, thromboemboli).
- Document comorbidities influencing the disease process (e.g. heart disease, kidney disease).
- A positive nasal swab for SARS-CoV-2 is not sufficient cause to include COVID-19 in the cause-of-death statement without gross or histologic features typical of COVID-19.
- Example cause of death statements:
- “Hypoxic respiratory failure due to diffuse alveolar damage due to sarcoV pneumonitis.”
- “Saddle pulmonary embolism due to DVT due to hypercoagulable state, due to SARsCoV viremia.”

- Image: Primary cause of death listed on death certificate from COVID-19 + autopsies. (Figure credit: Hooper 2024).
Recommended References
- Hooper JE, Sanchez H, Litovsky S, Lu ZA, Gabrielson EW, Padera RF, Steffensen T, Solomon IH, Gilbert A, Threlkeld KJ, Rapkiewicz AV, Harper H, Kapp ME, Schwerdt MK, Mount S, Wang Y, Lu R, Williamson AK. A Large Postmortem Database of COVID-19 Patients Can Inform Disease Research and Public Policy Decision Making. Arch Pathol Lab Med. 2024 Nov 1;148(11):e386-e393. doi: 10.5858/arpa.2023-0380-OA. PMID: 38452801.
- Hooper, J. E., Sanchez, H., Litovsky, S., Lu, Z. A., Gabrielson, E. W., Padera, R. F., … & Williamson, A. K. (2024). A Large Postmortem Database of COVID-19 Patients Can Inform Disease Research and Public Policy Decision Making. Archives of Pathology & Laboratory Medicine, 148(11), e386-e393.
- Yoshikawa A, Bychkov A. Acute Lung Injury/Diffuse Alveolar Damage. Pathology Outlines. Accessed 10/31/2024.
Additional References
- Hooper JE, Padera RF, Dolhnikoff M, da Silva LFF, Duarte-Neto AN, Kapp ME, Lacy JM, Mauad T, Saldiva PHN, Rapkiewicz AV, Wolf DA, Felix JC, Benson P, Shanes E, Gawelek KL, Marshall DA, McDonald MM, Muller W, Priemer DS, Solomon IH, Zak T, Bhattacharjee MB, Fu L, Gilbert AR, Harper HL, Litovsky S, Lomasney J, Mount SL, Reilly S, Sekulic M, Steffensen TS, Threlkeld KJ, Zhao B, Williamson AK. A Postmortem Portrait of the Coronavirus Disease 2019 (COVID-19) Pandemic: A Large Multi-institutional Autopsy Survey Study. Arch Pathol Lab Med. 2021 May 1;145(5):529-535. doi: 10.5858/arpa.2020-0786-SA. PMID: 33449998.
- Fotuhi M, Mian A, Meysami S, Raji CA. Neurobiology of COVID-19. J Alzheimers Dis. 2020;76(1):3-19. doi: 10.3233/JAD-200581. PMID: 32538857; PMCID: PMC7660990.
- Li Y, Xiao SY. Hepatic involvement in COVID-19 patients: Pathology, pathogenesis, and clinical implications. J Med Virol. 2020 Sep;92(9):1491-1494. doi: 10.1002/jmv.25973. Epub 2020 May 13. PMID: 32369204.
- Gagliardi I, Patella G, Michael A, Serra R, Provenzano M, Andreucci M. COVID-19 and the Kidney: From Epidemiology to Clinical Practice. J Clin Med. 2020 Aug 4;9(8):2506. doi: 10.3390/jcm9082506. PMID: 32759645; PMCID: PMC7464116.










{kind=link}