
Authors: Meagan Chambers MD & Harry Sanchez MD
Background
Pulmonary hypertension (PH) is defined by a mean pulmonary arterial pressure of > 20 mmHg at rest, as measured by right heart catheterization.
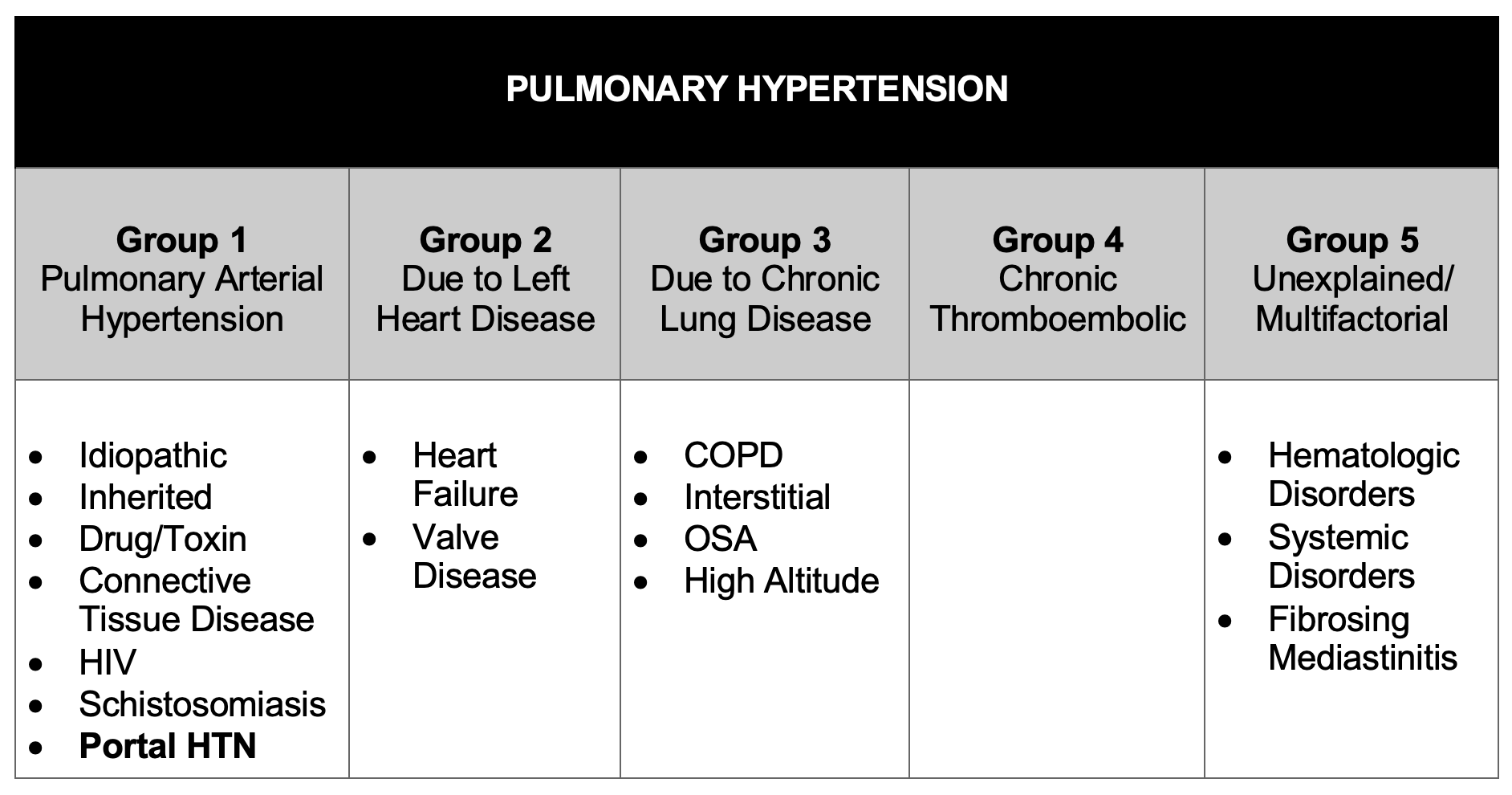
Based on the causative mechanism, the World Health Organization has divided cases of pulmonary hypertension into five groups:

- Right heart failure is the most common immediate cause of death.
Quick Tips at Time of Autopsy
Clinical History
- Pulmonary hypertension is a clinical diagnosis which is often known prior to death. The diagnosis and evaluation of pulmonary hypertension at autopsy requires the correlation of clinical, radiographic, and anatomic findings.
Internal examination
- Over time, the increased work occasioned by the increased vascular resistance leads to right atrial dilation, right ventricular dilatation, and right ventricular hypertrophy (cor pulmonale) which can be observed grossly at autopsy.
 Image: Right ventricular hypertrophy in a case of pulmonary hypertension. (Image credit: Meagan Chambers/University of Washington).
Image: Right ventricular hypertrophy in a case of pulmonary hypertension. (Image credit: Meagan Chambers/University of Washington).
- The increased pressure and shear stress on the pulmonary artery can be associated with pulmonary artery dilation and the formation of atherosclerotic plaques. The presence of atherosclerotic plaques on the pulmonary artery and its main branches in the absence of significant hyperlipidemia is highly suggestive of PH.

Image: atherosclerotic plaques in pulmonary arteries. (Image credit: Harry Sanchez/Yale University).
Quick Tips at Time of Histology Evaluation
- Identification of pulmonary arterial atherosclerosis on gross examination of the lungs should prompt detailed histologic evaluation of smaller vessels for features of pulmonary hypertensive vasculopathy including use of connective tissue stains such as trichrome, elastic and or pentachrome stains.
- In PAH, the increase in pulmonary artery pressure is caused by pathologic changes in the precapillary pulmonary small (50-500 um) arterial vessels. Characteristic histologic changes such as intimal hyperplasia, medial hypertrophy, plexiform lesions, and adventitial fibrosis are associated with increased vascular resistance.
- The right ventricular remodeling may be adaptive with concentric hypertrophy and minimal fibrosis, or maladaptive with eccentric hypertrophy and significant myocardial fibrosis. Therefore, the typical gross findings include a dilated pulmonary artery, cardiomegaly, and dilated right atrium and right ventricle.
- The right ventricular remodeling may be adaptive with concentric hypertrophy and minimal fibrosis, or maladaptive with eccentric hypertrophy and significant myocardial fibrosis. Therefore, the typical gross findings include a dilated pulmonary artery, cardiomegaly, and dilated right atrium and right ventricle.
- Acute histologic changes of increased atrial pressures include proteinaceous edema, hemosiderin laden macrophages, and distended perivascular lymphatics.
- The lung displays several common histopathologic features, characterized by remodeling of the three layers of the small pulmonary muscular arterioles
- Intima – intimal thickening due to endothelial cell proliferation; concentric laminar intimal proliferation and fibrosis; the vessel lumen may be occluded/obliterated; an elastic stain can highlight destruction/reduplication of the internal elastic lamina.
- Media – medial thickening due to smooth muscle cell hyperplasia.
- Adventitia – adventitial remodeling with collagen disruption and chronic inflammatory cells.

Image: Arteries and airways run together in the lungs – separate from veins. (This is in contrast to the rest of the body where arteries and veins run in parallel.) In normal lung, as in this photo, the caliber of the airway and the artery should be similar. This can be a useful baseline for comparing arterial alterations due to pulmonary hypertension. (Image credit: Meagan Chambers/Stanford University).
 Image: Intimal hyperplasia in a pulmonary artery (Image credit: Meagan Chambers/University of Washington).
Image: Intimal hyperplasia in a pulmonary artery (Image credit: Meagan Chambers/University of Washington).
- Arterialization of veins in the interlobular septa may also be seen.

Image: Trichrome (left) demonstrates arterialization of a vein in the interlobular septum including medial hypertrophy, prominent elastic laminae, and intimal fibrosis. (Image credit: Darren Salmi, Stanford University).
- Plexiform lesions are pathognomonic for PAH, resulting from intraluminal endothelialization of microaneurysms, which appear as tufts of capillaries spanning the lumina of arteries and sometimes extending out of the vessel. Plexiform lesions may also arise from vasa vasorum penetrating the wall structure of pulmonary vessels, with a “vessel arising from vessel” appearance. In situ thrombosis may be present. Importantly, the histopathologic findings of pulmonary vascular remodeling and plexiform lesions are indicative of the PAH clinical subcategory of PH (especially idiopathic and HIV related), but may also be seen in unrepaired congenital heart disease with left to right shunts (WHO group 2).

 Images (top and bottom): Plexiform lesions. (Image credit: Meagan Chambers/University of Washington).
Images (top and bottom): Plexiform lesions. (Image credit: Meagan Chambers/University of Washington).
- Capillaries demonstrate basement membrane thickening.
- Changes in the airspaces include thickening of the alveolar walls with type 2 pneumocyte hyperplasia.
- In larger airways there is bronchial smooth muscle hypertrophy.
Quick Tips at Time of Reporting
- The severity of pathologic changes of PAH does not correlate well with the patient’s clinical status or hemodynamic measurements.
- The immediate cause of death is usually right heart failure or respiratory failure:
- “Acute right heart failure due to pulmonary hypertension arteriopathy due to idiopathic pulmonary hypertension (WHO Group 1).”
- “Respiratory failure due to pulmonary hypertensive arteriopathy (WHO Group 1) due to portopulmonary hypertension due to cirrhosis of uncertain etiology, arising in the setting of a history of chronic alcohol use.”
Clinical Tidbits
- The average life expectancy without transplant is 3 years.
- One of the most common causes of PAH worldwide, schistosomiasis, is rarely seen in the United States. It is estimated that 80% of people with PAH live in the developing world.
Recommended References
- Sanchez, H. Pulmonary Hypertension. AUP2024. Autopsy Pathology Program. Northfield, IL: College of American Pathologists; 2023.
Additional References
- Hepinstall RH. Relation of hypertension to changes in the arteries. Prog Cardiovasc Dis 1974; 17:25-30.
- Vonk Noordegraaf A, Chin KM, Haddad F, et al. Pathophysiology of the right ventricle and of the pulmonary circulation in pulmonary hypertension: an update. Eur Respir J. 2019;53(1):1801900. Published 2019 Jan 24. doi:10.1183/13993003.01900-2018.










One Comment