
Authors: Meagan Chambers MD & Jody Hooper MD
Background
Pneumonia, sepsis, meningitis, peritonitis, and infective endocarditis rank among the top 10 diagnoses frequently missed in life. Consequently, antemortem microbiology testing is a vital tool in autopsy.
Positive postmortem cultures may indicate
- True Positive: An infectious organism, possibly unrelated to the cause of death
- False Positive
- Agonal Spread: Ischemic events during the agonal period or resuscitation may cause mucosal damage, allowing bacteria to breach surfaces. This theory, though once popular, lacks strong support in literature
- Postmortem Translocation: Bacterial movement from mucosal surfaces to the blood and internal organs postmortem
- Contamination: Unintended introduction of bacteria into samples
 Image: Brain with cavities from post-mortem spread of gas-forming bacteria in a case with a post-mortem interval of >90 hours. (Image credit: Meagan Chambers/University of Washington).
Image: Brain with cavities from post-mortem spread of gas-forming bacteria in a case with a post-mortem interval of >90 hours. (Image credit: Meagan Chambers/University of Washington).
Quick Tips at Time of Autopsy
Clinical History
- Review past medical records for completed (antemortem) microbiology studies
- Indications from the clinical history for postmortem testing
- Identification of the causative agent from a previously undiagnosed infection, including cases of sepsis
- Confirmation of an antemortem presumed infectious diagnoses. (If the causative pathogen is known prior to the autopsy, cultures may not be indicated, however they can be useful for evaluating the response to antibiotics)
- Sudden unexpected death, even without clinical suspicion or signs of infection
- In immunocompromised individuals, consider fungal and mycobacterial cultures
- Of note, an elevated C-reactive protein (CRP) level is correlated with a microbiologically related cause of death and, in the correct context, has been proposed as a guideline to initiate microbiological testing at autopsy (Christoffersen 2015)
External examination and internal examination
- To obtain the most accurate results, cultures are optimally taken in cases where the body is well preserved, promptly refrigerated, and autopsied within 48 hours postmortem
- Look for signs of infection like wound erythema, purulence, rashes, pulmonary consolidation, “milky” leptomeninges, etc.
- Ordering aerobic cultures are usually sufficient, but consider anaerobic bacteriology cultures when clinically indicated.
- Anaerobic bacterial infection can also be suggested by the presence of odor such as a “rotten-egg” odor or other foul smell
Ancillary Testing (i.e. taking cultures at autopsy)
- Generally, routine microbiological sampling of every autopsy is not indicated, nor supported by the literature
- Postmortem microbiology studies may be helpful in selected cases when properly performed and interpreted in light of the clinical context (see above) and anatomic findings (see above). To improve the diagnostic yield:
- Take cultures early in the autopsy procedure before performing extensive dissection. Internal organs should be sampled while they are in situ, immediately after opening the body
- Properly disinfect the site by searing with a hot spatula or disinfecting the surface using appropriate disinfectant (betadine/alcohol pretreatment)
- Collect sample using sterile needles/instruments and gloves
- For blood cultures, the subclavian vein is preferred over the jugular or femoral veins to minimize false positives. For the same reason, cardiac blood should only be collected when peripheral blood is not available
- Place the specimen in the proper medium
- Aerobic bacteriology – Swab or tissue in sterile container
- Anaerobic bacteriology – Swab or tissue in anaerobic media tube (obtained from microbiology)
- Of note, if blood is short, one anaerobic tube can be used for both aerobic and anaerobic microbiological studies
- Fungus and TB cultures – Swab or tissue in sterile container
- The samples collected should be sent to the laboratory within 2 hours when stored at room temperature and within 48 hours when refrigerated and in adequate transport media
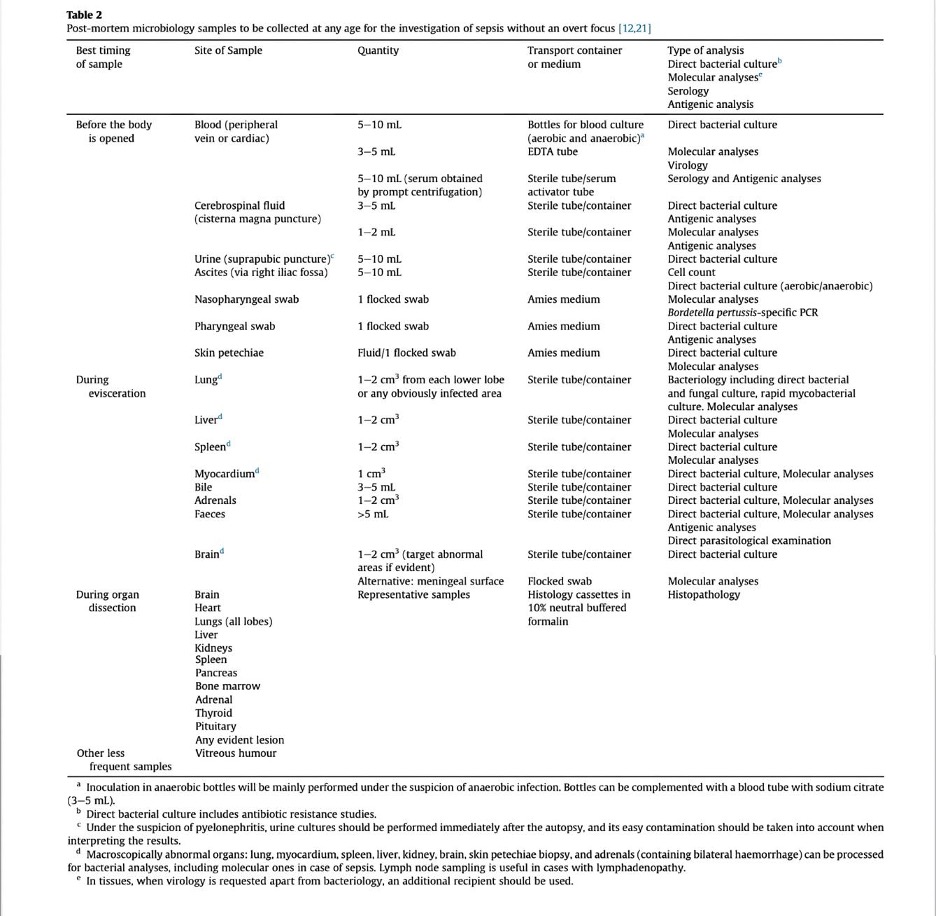
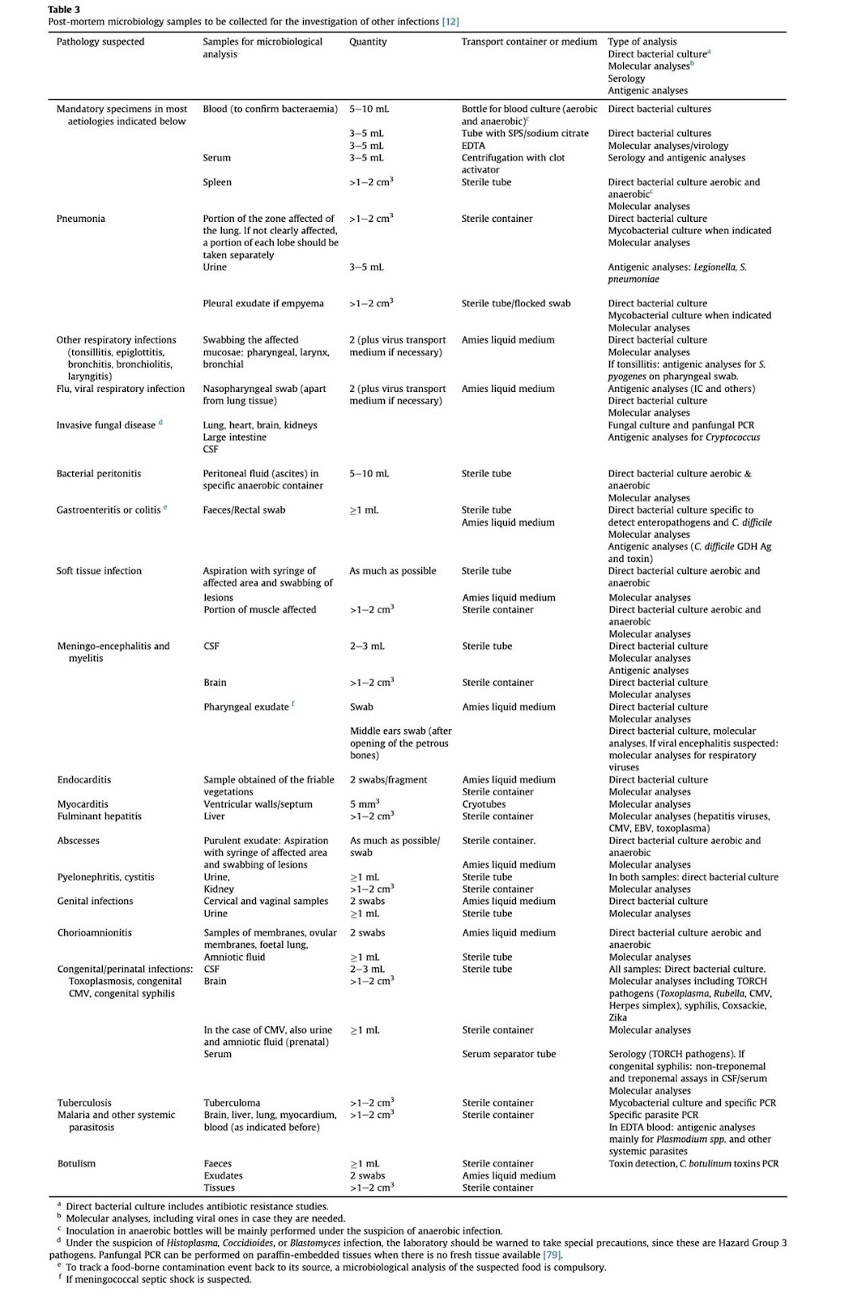
- Suggested protocols for sampling based on the specific clinical suspicion have been developed by the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Study Group of Forensic and Postmortem Microbiology (ESGFOR)
A quick summary is available here:

(Table Credit: Burton 2019)
- Additional tables are available from Fernández-Rodríguez 2019: Table 1 includes the specimens to be collected when there is the suspicion of sepsis without an overt focus, and Table 2 shows those to be collected when there is suspicion of specific infections
- Peripheral blood and spleen cultures are especially useful when the patient’s death occurred prior to obtaining adequate antemortem cultures
- Conservation of snap-frozen tissues from different locations permits later molecular microbiological analyses if, eventually, an infection is confirmed or suspected as the cause of death
- PCR testing can be useful in identifying pathogens of interest but multiplex (syndromic) molecular panels are more effective than broad- range PCR assays (such as the 16S Sanger sequencing) which is more susceptible to post-mortem translocation as contaminating bacteria can yield an unreadable mixture of sequences
- Post-mortem biochemical markers, even if non-specific, can be helpful in cases with negative post-mortem cultures. Procalcitonin (PCT) and C-reactive protein (CRP), have a role in differentiating infections from systemic inflammatory responses of non-infective origin (See Hassan 2022, Bode-Janisch 2013 for more information)
- In some cases, consultation from the CDC may be necessary. For assistance with this see this link: CDC Infectious Diseases Pathology Branch
Quick Tips at Time of Histology Evaluation
- Adequate histologic sampling is necessary to support the diagnosis and because there can be positive histology for organisms even in the face of negative cultures
- The significance of an organism on post-mortem cultures can be strongly supported by evidence of inflammation histologically
- In particular, aspirated particulate matter, bacteria, and yeast from the mouth in the absence of inflammation are more likely to be from perimortem aspiration, rather than representing a clinically significant aspiration/colonization
- In the case of indwelling devices or other non-sterile locations, infection vs colonization is an important distinction and evidence of inflammation on histology supports infection over colonization
- Inflammation may not be present in immunocompromised individuals
- Some infections have associated suggestive features which can help distinguish them from other infections
 Table: Histologic patterns of inflammation can suggest an organism. (Table credit: modified from Lucas 2012)
Table: Histologic patterns of inflammation can suggest an organism. (Table credit: modified from Lucas 2012)
Quick Tips at Time of Reporting
- Single organism cultures with histologic correlates (inflammation in the tissue sampled) is the best evidence of infection.
- Single organism cultures without a histologic correlate are also likely to be true positives, even without a histologic correlate, unless they are skin or oral commensal organisms.
- Gram negatives such as Staphylococcus are frequently present in postmortem cultures, but much less commonly the causative agent.
- Multiple organism cultures are much more likely to be contamination, but histologic correlation can swing these cases towards considering it a true pathogen.
- Multiple organism cultures without a histological correlate are the least likely to represent a true infection (but there are exceptions so clinical-pathologic correlation is always important).
- Quantitative evaluation can help clarify the role of the pathogen (death vs. contamination, or infection vs. colonization)
- Literature indicates that the isolation of single microbial agents with a high pathogenic capacity is to be considered as an important and significant finding for the diagnosis of the cause of death (Burton 2019 and Fernández-Rodríguez 2019)
- Several more or less commonly encountered microorganisms, such as N. meningitidis, Neisseria gonorrhoeae, Haemophilus influenzae, Salmonella species, Staphylococcus aureus, Streptococcus pneumoniae, b-hemolytic streptococci, Klebsiella species, Escherichia coli, Mycobacterium tuberculosis, members of the Enterobacteriaceae and C. albicans should, according to some authors, always be considered pathogens
- Retrieval of anaerobic microorganisms should be considered in the context of post-mortem translocation of anaerobic flora from the gastrointestinal trac
- For the cause of death, per CDC guidelines for death certification, include the organism name when possible
- e.g. “Community Acquired pan lobar pneumonia due to Streptococcus pneumoniae infection.”
Clinical Tidbits
- Nosocomial infections can be present in up to 10% of all hospitalized patients. See this table for a review of common nosocomial infections
- More relevant to forensics, post-mortem microbiome succession has been shown to be a foreseeable and time-dependent process; routine sampling for cultures has been proposed as a possible way to estimate postmortem interval using metagenomic sequencing and mass spectrometry
Recommended References
- Morris JA, Harrison LM, Partridge SM. Postmortem bacteriology: a re-evaluation. J Clin Pathol. 2006 Jan;59(1):1-9. doi: 10.1136/jcp.2005.028183. PMID: 16394274; PMCID: PMC1860254.
- Riedel S. The value of postmortem microbiology cultures. J Clin Microbiol. 2014 Apr;52(4):1028-33. doi: 10.1128/JCM.03102-13. Epub 2014 Jan 8. PMID: 24403308; PMCID: PMC3993482.
- Fernández-Rodríguez A, Burton JL, Andreoletti L, Alberola J, Fornes P, Merino I, Martínez MJ, Castillo P, Sampaio-Maia B, Caldas IM, Saegeman V, Cohen MC; ESGFOR and the ESP. Post-mortem microbiology in sudden death: sampling protocols proposed in different clinical settings. Clin Microbiol Infect. 2019 May;25(5):570-579. doi: 10.1016/j.cmi.2018.08.009. Epub 2018 Aug 24. PMID: 30145399
- Burton JL, Saegeman V, Arribi A, Rello J, Andreoletti L, Cohen MC, Fernandez-Rodriguez A; ESGFOR Joint Working Group of the European Society of Clinical Microbiology and Infectious Diseases (ESCMID) Study Group of Forensic and Postmortem Microbiology and the European Society of Pathology. Postmortem microbiology sampling following death in hospital: an ESGFOR task force consensus statement. J Clin Pathol. 2019 May;72(5):329-336. doi: 10.1136/jclinpath-2018-205365. Epub 2019 Jan 19. PMID: 30661015
Additional References
- Christoffersen S. The importance of microbiological testing for establishing cause of death in 42 forensic autopsies. Forensic Sci Int. 2015 May;250:27-32. doi: 10.1016/j.forsciint.2015.02.020. Epub 2015 Feb 28. PMID: 25769131; PMCID: PMC7130849
- Hassan J, Khan S, Zahra R, Razaq A, Zain A, Razaq L, Razaq M. Role of Procalcitonin and C-reactive Protein as Predictors of Sepsis and in Managing Sepsis in Postoperative Patients: A Systematic Review. Cureus. 2022 Nov 3;14(11):e31067. doi: 10.7759/cureus.31067. PMID: 36475186; PMCID: PMC9719405
- Bode-Jänisch S, Schütz S, Schmidt A, Tschernig T, Debertin AS, Fieguth A, Hagemeier L, Teske J, Suerbaum S, Klintschar M, Bange FC. Serum procalcitonin levels in the postmortem diagnosis of sepsis. Forensic Sci Int. 2013 Mar 10;226(1-3):266-72. doi: 10.1016/j.forsciint.2013.01.041. Epub 2013 Feb 19. PMID: 23434379
- Lucas SB. The autopsy pathology of sepsis-related death. Accessed 2023










{kind=link}
{kind=link}