
Authors: Meagan Chambers MD and Billie Fyfe MD
Background
Myocardial infarction (MI) is irreversible damage to the myocardium from decreased or complete cessation of blood flow upstream (a supply-demand mismatch).
Coronary artery atherosclerosis is the number one risk factor, responsible for 80%->90% of acute coronary syndromes. Other conditions intrinsic to the coronary arteries that cause MI include vasculitis, amyloidosis, coronary dissection, vasospasm, and emboli. Extrinsic conditions which can also lead to a perfusion/demand mismatch and subsequent ischemia include left ventricular hypertrophy, congenital heart disease, non-ischemic cardiac arrest (metabolic, arrhythmic, etc.), and impaired oxygen delivery (respiratory failure, anemia, hemorrhagic shock, etc.).
Acute and chronic complications of MI, many of which can be seen at autopsy, include myocardial rupture, mural thrombosis/embolism, pericarditis/Dressler syndrome, arrhythmias, cardiogenic shock, ischemic dilated cardiomyopathy/congestive heart failure, left ventricular aneurysm, and pulmonary hypertension.
Quick Tips at Time of Autopsy
Clinical history
- MI is usually suspected on the basis of ECG or laboratory workup but can also be an unsuspected finding.
- Check the records for pre-mortem diagnostics (such as troponin and coronary angiography).
External examination
- There are many physical signs which are associated with cardiovascular disease/atherosclerosis.
- Scars from prior surgical procedures (like coronary artery bypass grafting or pacemaker insertion) are evident externally and point towards a history of cardiovascular disease.
Internal examination
- If the case qualifies as sudden death then consensus guidelines for autopsy investigation of sudden cardiac death should be followed.
- See the atherosclerosis article for grossing and sampling recommendations for coronary arteries.
Recommended approach to grossing/sampling the heart
- Make a complete transverse (short-axis) cut of the heart at the mid-ventricular level and then further parallel transverse slices of ventricles at 1 cm intervals towards the apex.
- Triphenyl tetrazolium chloride (TTC) or nitro blue tetrazolium (NBT) can be used in the autopsy room for preliminary diagnosis of acute myocardial infarction.
- A 1-cm thick ventricular slice should be selected and immersed in neutral TTC solution for 15–20 min at 37 °C.
- The stain can be used to differentiate metabolically active and inactive tissues in early MI.
- It is only useful within 48 hours of death and on unfixed tissue
- Both stains change color in viable tissue; infarcted tissue will not discolor.
- Dissect the remainder of right and left ventricles in the basal half of the heart in the direction of the flow of blood. Complete the examination of atrial and ventricular septa, atrio-ventricular valves, ventricular inflows and outflows, and semilunar valves.
- Routine sections for histology should include
- Myocardium from a representative transverse slice of the ventricle including: the free wall of the left ventricle (anterior, lateral, and posterior), the ventricular septum (anterior and posterior), and the free wall of the right ventricle (anterior, lateral, and posterior), as well as right ventricular outflow tract.
- Left ventricular myocardial sections should include the papillary muscles.
- Retain one block from each atria.
- Myocardium from a representative transverse slice of the ventricle including: the free wall of the left ventricle (anterior, lateral, and posterior), the ventricular septum (anterior and posterior), and the free wall of the right ventricle (anterior, lateral, and posterior), as well as right ventricular outflow tract.
- For visible infarcts, sample the center and periphery of the lesion to capture the age variation of the infarct.
- Other macroscopic abnormalities should also be sampled
- In cases with stents or CABG, histological sampling of downstream myocardium is crucial to investigate the presence of myocardial injury.
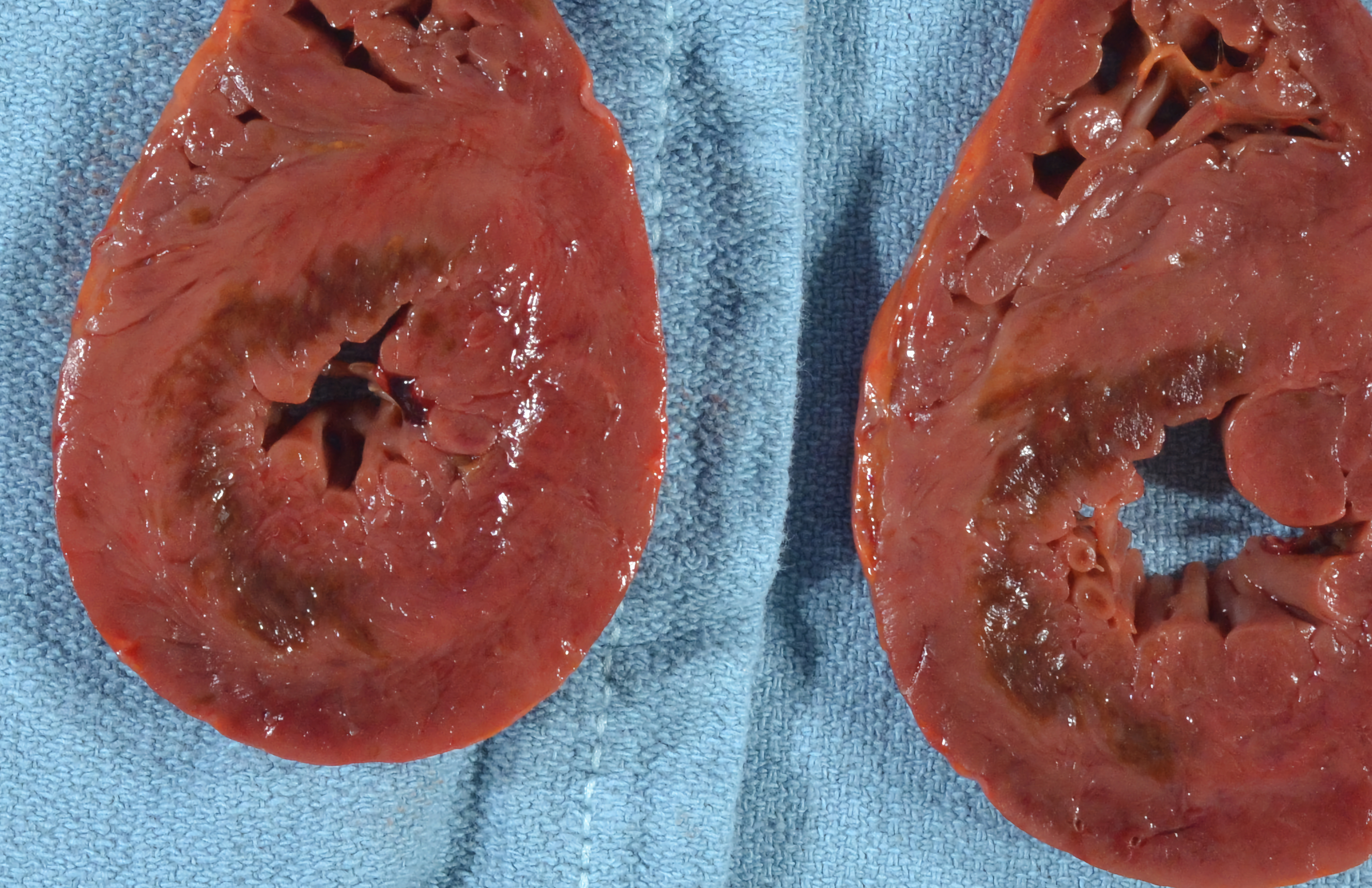
Macroscopic findings of MI
- Tissue changes from ischemia follow a general timeline
|
Time |
Gross Changes |
|
6-12 hours |
No changes |
|
12-24 hours |
No changes or subtle mottling, pallor or regional stiffness |
|
1-3 days |
Mottling with yellow-tan center (from leukocyte infiltration) |
|
3-7 days |
Yellow-tan center with hyperemic edges |
|
7-10 days |
Gelatinous early scar, grossly softened and depressed, hyperemic edges |
|
10-14 days |
|
|
3-8 weeks |
Grayish-white scar begins to form at edges and progresses to center |
|
7-8 weeks |
Cicatrization (fibroblast remodeling) may be complete |
|
8-12 weeks |
Grayish-white scar with early remodeling (wall thinning and chamber dilatation) |
(Table adapted from Nair and Caarmela)
- Revascularization/reperfusion (at any time) may result in a red-brown color (due to hemorrhage into ischemic tissues).
- The presence of a mural or occlusive thrombotic mass can be observed at autopsy in approximately 50–70% of sudden coronary deaths and is a reliable marker of myocardial ischemia, even in the absence of microscopically visible necrosis (Michaud 2019).
- Mural thrombi are most common in anteroapical MIs and are a risk factor for systemic embolization.
Grossly identifiable complications of MI
- Myocardial rupture: occurs 7-10 days post infarct due to weak granulation tissue, usually in the context of a left ventricular wall infarct. An intraventricular rupture leads to right/left shunting while a free wall rupture leads to hemoperitoneum.
- Pericarditis/Dressler’s syndrome: differing in their timeline and underlying etiology, both appear grossly as a fine granular layer on the epicardial surface described as a “bread and butter” appearance.
- Ischemic dilated cardiomyopathy/congestive heart failure: a dilated, globose heart
- Left ventricular aneurysm (see image below).
 Image: Chronic, left ventricular aneurysm with dense endocardial fibrosis. (Image credit: Dr. Corine Fligner, University of Washington)
Image: Chronic, left ventricular aneurysm with dense endocardial fibrosis. (Image credit: Dr. Corine Fligner, University of Washington)
Ancillary testing
- High-sensitivity troponin testing can detect myocardial injury at ~3 hours and remains stable after death (should ante-mortem samples not be available).
- The magnitude of the troponin level does not correlate well with cause of death (i.e. a very high troponin level does not mean the MI was fatal).
- Low troponin in pericardial fluid does rule out significant heart damage (González-Herrera 2016).
- If you are considering testing Troponin at autopsy, see this excellent article for a full review of postmortem testing.
- In cases of stenting or CABG-related MI, post-mortem coronary angiography has been recommended, when available.
- If stents are present, they should be visually inspected for a thrombus. If light does not pass through the lumen then the specimen should be sent for consultation to a laboratory for laser cutting which will allow the thrombus to be viewed histologically with intact relationship to the stent.
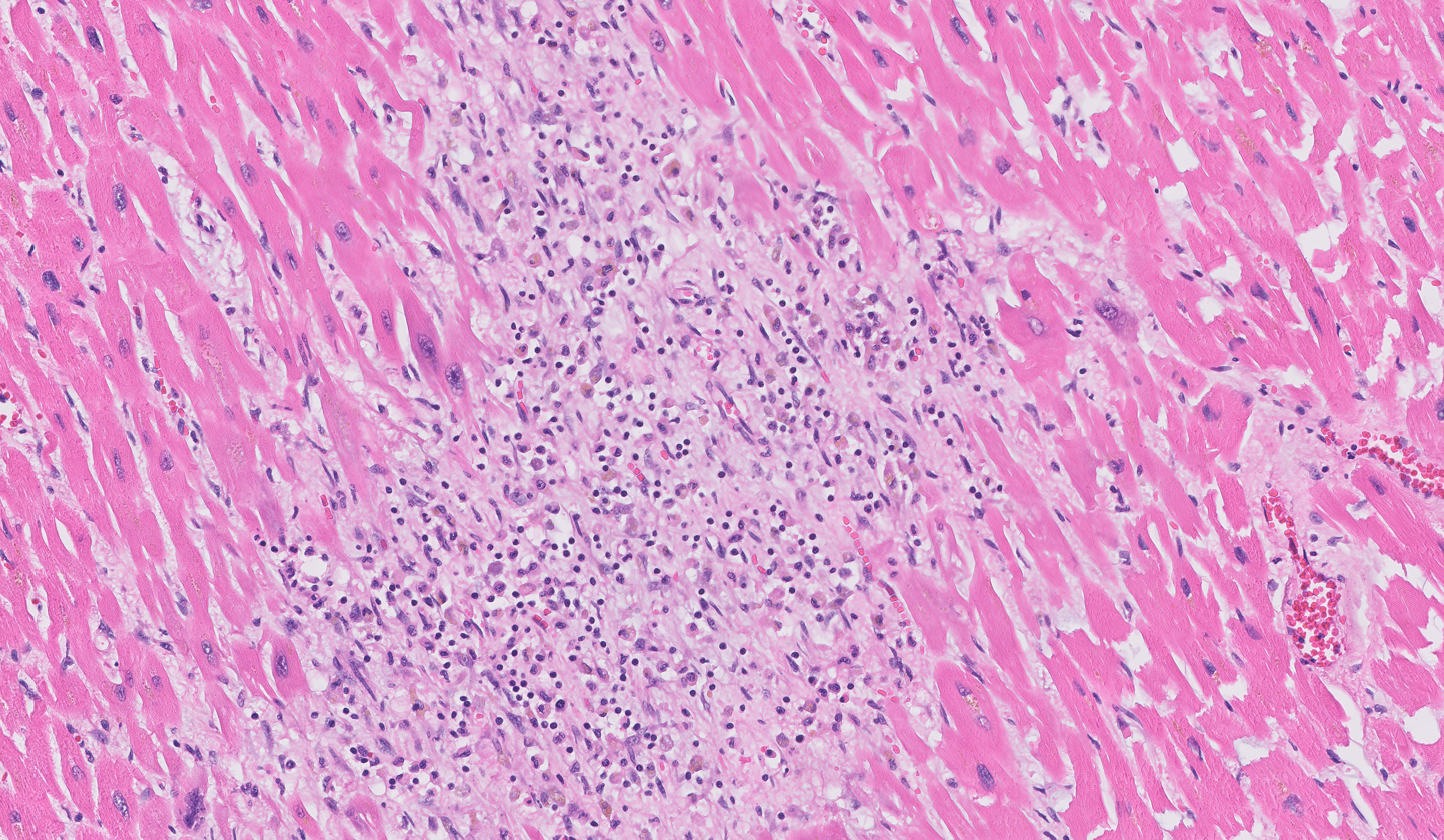
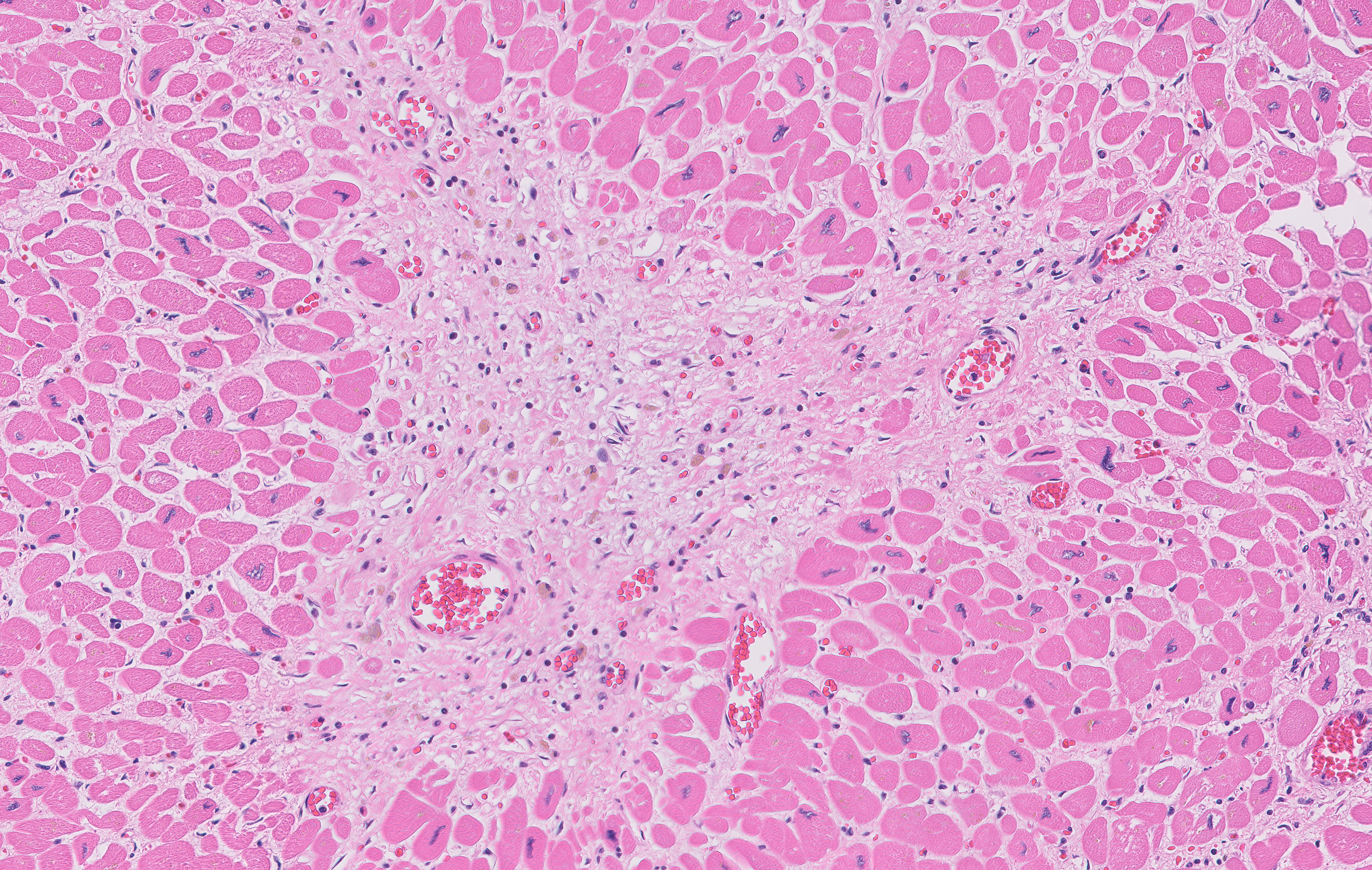
Quick Tips at the Time of Histology Evaluation
- Myocardial necrosis spreads outward from the subendocardium to the subepicardial myocardium
- The papillary muscles are an excellent screening section to evaluate clinically unsuspected demand ischemia
- H&E changes follow a general timeline…
| Time | Histologic Changes |
| 4-6 hours | Margination of neutrophils. After 4 hours (variable), myocytes may appear wavy and elongated, interstitial edema |
| 8-12 hours | Neutrophil extravasation into myocardial tissue |
| 1-3 days | Hypereosinophilic fibers, nuclear pyknosis, coagulation necrosis (loss of nuclei/striations), colliquative myocytolysis, edema, hemorrhage, myocyte contraction bands, and more neutrophils |
| 3-7 days | Myocyte loss, karyorrhexis of neutrophils (“nuclear dust”), early phagocytosis by macrophages at infarct border, early granulation tissue and capillary proliferation at the edges |
| 7-10 days | Well-developed phagocytosis with distended macrophages |
| 10-14 days | Well-established granulation tissue with new blood vessels and fibroblast infiltration, hemosiderin-laden macrophages, some plasma cells/eos, neutrophils are gone |
| 2-8 weeks | Increased collagen deposition with decreased cellularity |
| > 2 months | Dense collagenous (“healed”) scar |
(Table credit: adapted from Nair and Caarmela).
 Image: Remote myocardial infarction of the septum with replacement fibrosis (blue on trichrome stain) and lipomatous metaplasia. (Image credit: Dr. Corine Fligner, University of Washington)
Image: Remote myocardial infarction of the septum with replacement fibrosis (blue on trichrome stain) and lipomatous metaplasia. (Image credit: Dr. Corine Fligner, University of Washington)
- If revascularization occurs (spontaneously or therapeutically) features of reperfusion injury may be present including
- Contraction band necrosis
- Marked erythrocyte extravasation/hemorrhage
- Small vessels with thrombi or atheroemboli
- Immunohistochemistry
- Staining for C4d may be positive in acutely ischemic myocytes due to complement activation, possibly earlier than it can be detected on H&E (possibly <12 hours, but the exact timing is unknown).
- Other guidelines have suggested a combination of fibronectin and C5b-9 immune stains. C5b-9 staining is more sensitive and specific than fibronectin staining, but fibronectin positivity starts earlier than C5b-9.
- Desmin staining will highlight necrosis in blue (after 24-48 hours post infarction).
 Image credit: Michaud 2019
Image credit: Michaud 2019
- Identifying the underlying cause of the MI is an important component of the autopsy. The chart below reviews some of the histologic findings which can help elucidate the underlying cause of ischemic damage.
| Causes of Myocardial Infarction and Their Gross/Histologic Correlates at Autopsy | |
| Atherosclerosis | Ruptured and unruptured/stable plaques can be responsible. See atherosclerosis for more information. |
| Coronary Spasm | There are no distinctive gross or histologic hallmarks. Can look for diffuse intimal and medial thickening with low lipid or calcium content, negative remodeling and small luminal cross-sections which predispose to spasm, especially in association with microscopic evidence of ischemia. In the history, drugs (incl. cocaine, amphetamines, androgenic anabolic steroids, chemotherapy), physical and mental stress and release of vasoconstrictor agents by activated platelets (mural thrombus) are precipitating factors. Very rarely, CAS can occur in the setting of allergic/hypersensitivity reactions, which is known as Kounis Syndrome and histologically characterized by the presence of eosinophils. |
| Small Vessel Disease | Microvascular disease is seen in hypertrophic and dilated hearts, preferentially in the subendocardial areas of the myocardium, as well as diabetic and hypertensive hearts, although the histologic findings are subtle. In transplanted hearts, SVD can be caused by widespread small vessel stenosis due to cardiac allograft vasculopathy. |
| Microvascular embolization | Widespread atherosclerotic emboli are an uncommon cause of acute MI, although they may result in microinfarctions occurring scattered through the myocardium. These may also have different acute/subacute/chronic timelines simultaneously. Microvascular embolization can also occur in patients with atrial fibrillation, prosthetic heart valves, infective endocarditis or cardiac myxoma. |
| Stent thrombosis/complications | Both acute and late stent occlusion events are rare. Neoatherosclerosis of the stent has been described and should be evaluated at autopsy. Microvascular coronary embolization with thromboembolic materials distal to a thrombosed epicardial plaque can be found at autopsy in patients who died of MI especially those with primary percutaneous coronary intervention (PCI) for acutely thrombosed plaques. |
| Adapted from Michaud 2019 | |
Quick Tips at Time of Reporting
- A consensus statement has defined five categories of myocardial infarction which may be a useful descriptive tool at autopsy (see Michaud 2019 for a summary).
- Example cause of death statements
- Myocardial infarct due to coronary artery atherosclerosis. Contributing conditions include diabetes and smoking.
- Myocardial infarct due to coronary artery dissection arising in pregnancy.
- Myocardial infarct due to coronary artery involvement in Kawasaki disease.
Recommended References
- Michaud K, Basso C, d’Amati G, Giordano C, Kholová I, Preston SD, Rizzo S, Sabatasso S, Sheppard MN, Vink A, van der Wal AC; Association for European Cardiovascular Pathology (AECVP). Diagnosis of myocardial infarction at autopsy: AECVP reappraisal in the light of the current clinical classification. Virchows Arch. 2020 Feb;476(2):179-194. doi: 10.1007/s00428-019-02662-1. Epub 2019 Sep 14. PMID: 31522288; PMCID: PMC7028821.
- Carmela D. Tan, M.D, and E Rene Rodriguez, M.D. Myocardial Infarction. Website Accessed 8/2023.
- Additional gross and histologic images are available on the University of Utah’s Internet Pathology Laboratory. Website accessed 10/2023.
- Sacco MA, Gualtieri S, Grimaldi G, Monterossi MD, Aquila VR, Tarallo AP, Verrina MC, Ranno F, Gratteri S, Aquila I. The Role of Cardiac Troponins in Postmortem Diagnosis of Myocardial Ischemia: A Systematic Review. Int J Mol Sci. 2024 Dec 26;26(1):105. doi: 10.3390/ijms26010105. PMID: 39795962; PMCID: PMC11719723.
Additional Citations
- Barth RF, Kellough DA, Allenby P, Blower LE, Hammond SH, Allenby GM, Buja LM. Assessment of atherosclerotic luminal narrowing of coronary arteries based on morphometrically generated visual guides. Cardiovasc Pathol. 2017 Jul-Aug;29:53-60. doi: 10.1016/j.carpath.2017.05.005. Epub 2017 May 30. PMID: 28622581.
- González-Herrera L, Valenzuela A, Ramos V, Blázquez A, Villanueva E. Cardiac troponin T determination by a highly sensitive assay in postmortem serum and pericardial fluid. Forensic Sci Med Pathol. 2016 Jun;12(2):181-8. doi: 10.1007/s12024-016-9749-1. Epub 2016 Mar 8. PMID: 26956978.
- Stone JR, Basso C, Baandrup UT, Bruneval P, Butany J, Gallagher PJ, Halushka MK, Miller DV, Padera RF, Radio SJ, Sheppard MN, Suvarna K, Tan CD, Thiene G, van der Wal AC, Veinot JP. Recommendations for processing cardiovascular surgical pathology specimens: a consensus statement from the Standards and Definitions Committee of the Society for Cardiovascular Pathology and the Association for European Cardiovascular Pathology. Cardiovasc Pathol. 2012 Jan-Feb;21(1):2-16. doi: 10.1016/j.carpath.2011.01.001. Epub 2011 Feb 24. PMID: 21353600.
- Nair V and Miller D. Acute Myocardial Infarction. ExpertPath. Accessed 2023 (login required).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}