Authors: Duy Doan MD & Jared Hassler MD
Background
Arrhythmogenic Right Ventricular Cardiomyopathy (ARVC) is an autosomal dominant genetic disorder marked by ventricular tachycardias, sudden cardiac death (SCD), and progressive deterioration of ventricular function.
It is the second most common cause of sudden cardiac death (SCD) in individuals under 35, in association with findings of hypertrophic cardiomyopathy. Arrhythmogenic right ventricular cardiomyopathy is more prevalent in males than in females. While the disease primarily affects the right ventricle (RV), it can also involve both ventricles.
Arrhythmogenic right ventricular cardiomyopathy arises from defects in desmosomes, essential components of cellular junctions (intercalated disk) crucial for maintaining cardiomyocyte stability and integrity. Mutations in genes coding for desmosome proteins result in dysfunctional cellular junctions, leading to structural alterations in the right ventricle. These changes predispose individuals to life-threatening ventricular arrhythmias and right heart failure.
- Five desmosomal genes (PKP2, DSP, DSG2, DSC2, and JUP)
- Three non-desmosomal genes (TMEM43, DES, and PLN). These non-desmosomal gene variants have been shown to impact desmosomal protein expression or function.
Quick Tips at Time of Autopsy
Clinical History
- Family history can be significant: unexplained sudden deaths among first-degree relatives.
- Palpitations or syncope can be attributed to underlying ventricular arrhythmias.
- Sudden cardiac death either at rest or during exercise.
- Right heart failure: peripheral edema, jugular venous distension, hepatosplenomegaly or hepatic pulsation, ascites, S3 gallop, and a right ventricular heave.
- Review the decedent’s previous EKG or Holter EKG (24-hour portable EKG) results: T-wave inversions in leads V1–V3, epsilon waves, unsustainable or sustainable ventricular tachycardias. (Please see “The 2010 modified Task Force Criteria”)
- Review the decedent’s previous echocardiography: right ventricle global dilatation and dysfunction, regional wall-motion abnormalities like systolic akinesia, dyskinesia, or diastolic bulging
- Review the decedent’s previous endocardial biopsies. TAB Arrhythmogenic Right Ventricle CardiomyopathyTAB Arrhythmogenic Right Ventricle Cardiomyopathy
 Image: ECG in a patient with ARVC revealing T-wave inversion in V1 through V4. (Image credit: Marcus 2010).
Image: ECG in a patient with ARVC revealing T-wave inversion in V1 through V4. (Image credit: Marcus 2010).
External examination
- Syncope-related injuries
- Peripheral edema and ascites can be seen, however, they are not specific to right heart failure
- Evidence of CRP-related injuries
- If palmoplantar keratosis and woolly hair are observed, these may indicate syndromic conditions such as Naxos disease or Carvajal syndrome.
- Naxos disease, an autosomal recessive cardiocutaneous syndrome, was first described in the Greek island of Naxos, characterized by triads of ARVC, palmoplantar keratosis, and Woolly hair. Mutations in the plakoglobin gene (JUP) (a desmosomal gene) were identified, affecting both myocardial and epidermal tissues due to shared desmosomal abnormalities.
- Carvajal syndrome, also an autosomal recessive disorder commonly found in Ecuador, shares clinical features similar to Naxos disease. It is caused by mutations in the desmoplakin gene (DSP) (also a desmosomal gene).
 Images: (Left) Posterior view of the head of a patient with Carvajal syndrome showing the characteristic woolly hair. (Right) Plantar keratoderma of a patient with Carvajal syndrome. (Image credits: Prompona 2007).
Images: (Left) Posterior view of the head of a patient with Carvajal syndrome showing the characteristic woolly hair. (Right) Plantar keratoderma of a patient with Carvajal syndrome. (Image credits: Prompona 2007).
Internal examination
- Right ventricle enlargement can be seen. The right ventricle wall can be thickening or thinning with aneurysm depending on the disease variants.
- Grossly fatty infiltration of the right ventricle, ventricular septum, or left ventricle. The most commonly affecting specific areas known as the triangle of dysplasia: the anterior right ventricular outflow tract, apex, and inferoposterior wall.
- Myocardium between epicardial and endocardial layers in areas of the RV wall assessed by transillumination with a source of light introduced inside the RV chamber.
 Image: Gross examination shows dilated cardiomyopathy in this case of ARVC. (Image credit: Duy Doan/Temple University).
Image: Gross examination shows dilated cardiomyopathy in this case of ARVC. (Image credit: Duy Doan/Temple University).
 Image: The formalin-fixed heart, viewed in cross-section, revealed full-thickness fatty infiltration near the right ventricular outflow tract, specifically within the triangle of dysplasia. (Image credit: Duy Doan/Temple University).
Image: The formalin-fixed heart, viewed in cross-section, revealed full-thickness fatty infiltration near the right ventricular outflow tract, specifically within the triangle of dysplasia. (Image credit: Duy Doan/Temple University).
Ancillary Testing
- Genetic testing for desmosome gene mutations can be performed
Quick Tips at Time of Histology Evaluation
- Identification of abnormally fatty right ventricle on gross examination should prompt extensive sampling evaluation of the right ventricle, particularly from the triangle of dysplasia as mentioned earlier, including the use of special stains such as trichrome to look for increasing fibrosis
- There are two histological variants of ARVC: the fatty variant and fibrofatty variant.
The fatty variant:
- Adipose tissue infiltrates the endocardium with minimal fibrous tissue
- Predominantly confined to the right ventricle while sparing the septum and left ventricle
- Potentially leading to increased ventricular wall thickness
The fibrofatty variant:
- Extensive fibrosis and fatty tissue replacement are often accompanied by inflammatory cell infiltrates such as T-lymphocytes and cardiomyocyte death.
- The right ventricular wall may become thinner and translucent, with a risk of forming aneurysms.
- The fibrofatty variant can involve the septum and left ventricle, making it more prone to electrical instability and sudden death.
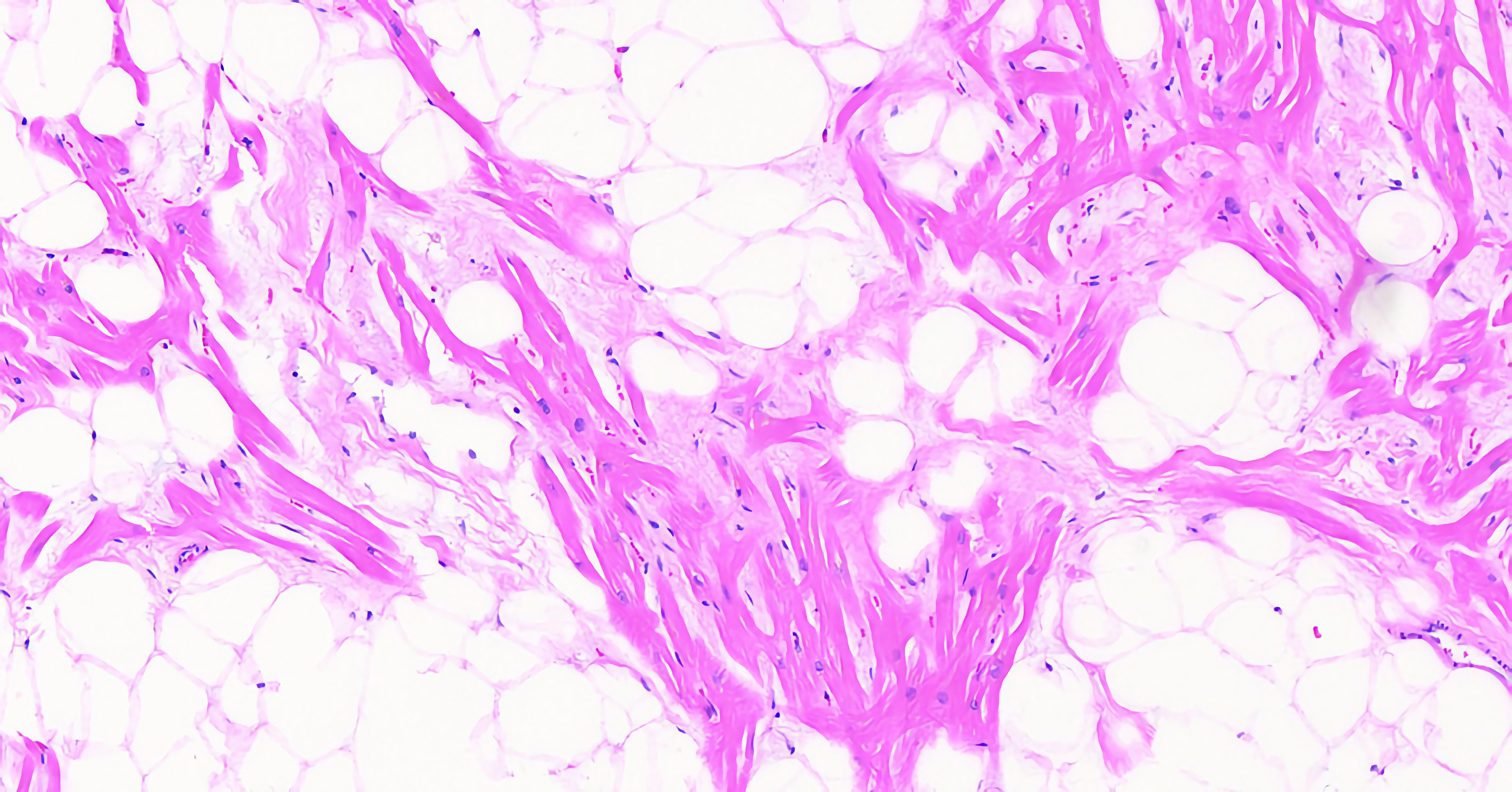
 Image: Right ventricle wall with fibrofatty replacement (H&E, 200x). (Image credit: Duy Doan/Temple University).
Image: Right ventricle wall with fibrofatty replacement (H&E, 200x). (Image credit: Duy Doan/Temple University).
 Image: Right ventricle wall with fibrofatty replacement (Trichrome, 200x). (Image credit: Duy Doan/Temple University).
Image: Right ventricle wall with fibrofatty replacement (Trichrome, 200x). (Image credit: Duy Doan/Temple University).
- ARVC should be distinguished from both fatty infiltration of the right ventricle and adipositas cordis (shown in the following table).
| ARVC | Adipositas Cordis | Fatty infiltration of the right ventricle | |
| Demographic | Male > Female | Female>Male, obese | Independent of sex and body weight |
| Fat centric | Infiltrates all the way from epicardium to endocardium | Exclusively involves epicardium | Epicardium, may separate myocardium but mostly surrounds blood vessels and nerves |
| Fibrosis | Two variants:
|
– | – |
| Inflammation |
+/- |
– |
– |
| Myocardial damage |
+ |
– |
– |
| Right ventricle wall thickness | Thickening (pseudo-hypertrophy) in fatty variant
Thinning in fibrofatty variant |
Normal | Normal |
 Image: ARVC in the right ventricle. Low power demonstrates diffuse fatty infiltration but also areas concerning for fibrosis and inflammation. (Image credit: Meagan Chambers/Stanford Hospital).
Image: ARVC in the right ventricle. Low power demonstrates diffuse fatty infiltration but also areas concerning for fibrosis and inflammation. (Image credit: Meagan Chambers/Stanford Hospital).
 Image: Close up of the above case of ARVC highlighting the fatty infiltration and surrounding fibrosis which is quite extensive. (Image credit: Meagan Chambers/Stanford Hospital).
Image: Close up of the above case of ARVC highlighting the fatty infiltration and surrounding fibrosis which is quite extensive. (Image credit: Meagan Chambers/Stanford Hospital).
 Image: Close up of the same case demonstrating some acute inflammation in areas of dense fibrosis. (Image credit: Meagan Chambers/Stanford Hospital).
Image: Close up of the same case demonstrating some acute inflammation in areas of dense fibrosis. (Image credit: Meagan Chambers/Stanford Hospital).
Quick Tips at Time of Reporting
- Cause of death: arrhythmogenic right ventricular cardiomyopathy
- There are ongoing debates surrounding this issue. Specifically, concerning the fatty variant, certain researchers argue that the presence of fatty replacement in the right ventricle alone, without accompanying fibrosis or inflammation, might not meet the criteria for diagnosing ARVC. In such instances, describing the diagnosis as “sudden death in a heart with extensive RV fatty infiltration” could be more appropriate. This terminology avoids suggesting a direct cause-and-effect relationship and allows for the exploration of alternative explanations for the cause of death. As for the fibrofatty variant, some experts propose that extensive replacement fibrosis and inflammation may be linked to previous viral myocarditis rather than indicating true ARVC.
Recommended References
- Marcus FI, McKenna WJ, Sherrill D, Basso C, Bauce B, Bluemke DA, Calkins H, Corrado D, Cox MG, Daubert JP, Fontaine G, Gear K, Hauer R, Nava A, Picard MH, Protonotarios N, Saffitz JE, Sanborn DM, Steinberg JS, Tandri H, Thiene G, Towbin JA, Tsatsopoulou A, Wichter T, Zareba W. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: proposed modification of the Task Force Criteria. Eur Heart J. 2010 Apr;31(7):806-14. doi: 10.1093/eurheartj/ehq025. Epub 2010 Feb 19. PMID: 20172912; PMCID: PMC2848326.
- Graziano F, Zorzi A, Cipriani A, De Lazzari M, Bauce B, Rigato I, Brunetti G, Pilichou K, Basso C, Perazzolo Marra M, Corrado D. The 2020 “Padua Criteria” for Diagnosis and Phenotype Characterization of Arrhythmogenic Cardiomyopathy in Clinical Practice. J Clin Med. 2022 Jan 5;11(1):279. doi: 10.3390/jcm11010279. PMID: 35012021; PMCID: PMC8746198.
- Corrado D, Zorzi A, Cipriani A, Bauce B, Bariani R, Beffagna G, De Lazzari M, Migliore F, Pilichou K, Rampazzo A, Rigato I, Rizzo S, Thiene G, Perazzolo Marra M, Basso C. Evolving Diagnostic Criteria for Arrhythmogenic Cardiomyopathy. J Am Heart Assoc. 2021 Sep 21;10(18):e021987. doi: 10.1161/JAHA.121.021987. Epub 2021 Sep 17. PMID: 34533054; PMCID: PMC8649536.
- Basso C, Thiene G. Adipositas cordis, fatty infiltration of the right ventricle, and arrhythmogenic right ventricular cardiomyopathy. Just a matter of fat? Cardiovasc Pathol. 2005 Jan-Feb;14(1):37-41. doi: 10.1016/j.carpath.2004.12.001. PMID: 15710290.
- Thiene G, Nava A, Corrado D, Rossi L, Pennelli N. Right ventricular cardiomyopathy and sudden death in young people. N Engl J Med. 1988 Jan 21;318(3):129-33. doi: 10.1056/NEJM198801213180301. PMID: 3336399.
- Burke AP, Farb A, Tashko G, Virmani R. Arrhythmogenic right ventricular cardiomyopathy and fatty replacement of the right ventricular myocardium: are they different diseases? Circulation. 1998 Apr 28;97(16):1571-80. doi: 10.1161/01.cir.97.16.1571. PMID: 9593562.
- Carvajal-Huerta L. Epidermolytic palmoplantar keratoderma with woolly hair and dilated cardiomyopathy. J Am Acad Dermatol. 1998 Sep;39(3):418-21. doi: 10.1016/s0190-9622(98)70317-2. PMID: 9738775.
Additional References
- Protonotarios N, Tsatsopoulou A. Naxos disease and Carvajal syndrome: cardiocutaneous disorders that highlight the pathogenesis and broaden the spectrum of arrhythmogenic right ventricular cardiomyopathy. Cardiovasc Pathol. 2004 Jul-Aug;13(4):185-94. doi: 10.1016/j.carpath.2004.03.609. PMID: 15210133.
- Fontaine G, Fontaliran F, Frank R. Arrhythmogenic right ventricular cardiomyopathies: clinical forms and main differential diagnoses. Circulation. 1998 Apr 28;97(16):1532-5. doi: 10.1161/01.cir.97.16.1532. PMID: 9593556.









